To Help Trans-Identifying Kids, Follow The Science
By Anonymous

Much is being learned
As a STEM researcher and a lifelong liberal democrat, I fervently hold that young trans-identifying people or those with gender dysphoria (distress with their sexed body) deserve the best treatment that science and medicine can offer. I believed until recently that gender dysphoria and its optimal treatments were well understood, and that the biggest problem was that young people couldn’t access the medical interventions they needed. As advised by many of the liberal organizations I belong to, I signed petitions to representatives and organizations in support of what I thought was necessary supportive treatment for these young vulnerable people.
My heart was—and is—in the right place. But my information was wrong.
After gender dysphoria impacted my inner circle, I began studying the scientific literature to learn more. As I pored over published papers, comparing their assertions with the evidence offered in support, I became increasingly alarmed. A study would find only an association with an intervention (association means you do not know whether the intervention caused an outcome) and then imply the intervention caused benefit, for example:[1] “access to this treatment is associated with lower odds of lifetime suicidal ideation. This study strengthens recommendations by […] for this treatment to be made available for transgender adolescents who want it.” The abstract of another study highlighted people reporting they improved from medication, but didn’t mention that their corresponding clinician reports did not find this improvement, while yet another study showed impressive plots of benefit with medical intervention, even though once one took into account accompanying mental health interventions for these conditions (hidden in a table at the end), only one of their 12 measures had a statistically significant improvement.
The list goes on. This essay is an attempt to share with you what I’ve learned. Something has gone very wrong in our attempt to help these young people, so much so that too many have been badly harmed—and I hope to explain why. (If you prefer videos, you can watch this excellent documentary, one of many).
It turns out that gender dysphoria is not well understood. Gender dysphoria is a set of symptoms, several of which are based upon gender stereotypes. One of the symptoms is discomfort that can be painfully severe. But having gender dysphoria does not on its own indicate the best treatment to resolve it for the long term. (Successful short-term relief is insufficient–think opioids.) There appears to be several kinds of gender dysphoria. For instance, although some people report having identified as trans throughout their lives, for many, being trans-identified or having gender dysphoria is temporary. You likely have not heard (I had not) that most kids in past studies who had gender dysphoria before puberty, and who weren’t socially or medically transitioned, had their gender dysphoria disappear by going through puberty. Or that it’s unknown why gender dysphoria arises or when it might remain long-term for trans-identified and gender-dysphoric adolescents—with or without medical intervention! Most importantly, there is no reliable way to establish in which young person gender dysphoria might or might not be transient and practitioners don’t agree on how to best help those who have it.
It is known that transient gender dysphoria can develop in many ways, including:
- Being pregay or having internalized homophobia. Medical intervention harmed Ritchie and Keira, who had such conditions.
- Being queer or non-stereotypical. Medical intervention harmed Shapeshifter
- Sexual harassment/trauma. Medical intervention harmed Sinead
- Being on the spectrum. Medical intervention hurt Laura
- Having a combination of mental health issues. Medical intervention hurt Michelle
- Being unusual, being bullied. Medical intervention hurt Abel and Frank
- Having anxiety, social anxiety or self hatred. Medical intervention hurt Stephen
- Being anorexic. Johanna realized anorexia could be causing her gender dysphoria, not vice versa, while medical intervention hurt Prisha
- Being drawn in through social networks and guilt about privilege. Medical transition hurt Helena.
- Difficulty with growing into a sexual adult (sometimes related to issues with parents), anxiety about approaching adulthood, or other reasons (e.g., “If you don’t fit in, that’s a sign you are trans. If you don’t like your body, then that’s a sign that you are trans.”).
Those who sought medical transition and later realized that it harmed them have reported that, at the time, they believed that these interventions were what they needed, and that they were likely another Caitlin Jenner or Dr Rachel Levine. Some detransitioners believed at the time that medical intervention could actually change their sex. But most were not told about cases like the ones above—or that for some young people gender dysphoria goes away simply by maturing, or by better understanding themselves and/or by dealing with other serious mental stresses. A therapist who treated gender dysphoric adults in the NHS for over a decade (using group therapy) observed that:
“I typically found that after anything from 6-12 months in the group the initial Gender Dysphoria had been completely resolved. The Gender Dysphoria was a solution that their mind had come up with to make sense of the confusion, which they happened to find in a gender framework. Once they had come to the conclusion that gender was the framework they had stuck with it.
In the world of affirmation or denial, it had rarely been challenged until they entered the group. Often the patients remained in the group long after the Gender Dysphoria had been resolved and found themselves to be in a useful therapeutic role for others coming in.”
In addition, there’s been a recent huge rise in the number of young people who have gender dysphoria or are trans-identifying (for example, the number of UK adolescents seeking treatment rose by a factor of over 25 in 7 years! [2]). Clinicians don’t agree on the reasons for this rise. These adolescents, more frequently girls, appear to be a different group than the earlier ones studied: mostly older men or kids under ten, mostly boys, the majority of which outgrew it.[3] Some researchers postulate social interactions as a factor (some supporting evidence has been found); others claim the quick large rise is just greater social acceptance of trans people but have not shown that this explanation fully accounts for the large numbers. In particular, several of the young people mentioned above, and others, developed gender dysphoria when someone suggested being trans was a reason for other distress. Many teachers, therapists, and others don’t realize that encouraging young people to ruminate on their gender and celebrating those who have “interesting” genders could end up causing harm. Many do not even know themselves that being trans can be temporary, and/or believe (and sometimes claim to parents) the falsehood that kids will commit suicide unless medically altered or treated as another sex. It cannot be repeated enough: studies have not established that medical intervention, social transition, or affirmation prevent suicide, or that not doing these things causes suicide (it is not only false but dangerously irresponsible to tell young people or their parents otherwise, as suicide is suggestible).
Here’s a schematic of some ways into gender dysphoria and some things that might then happen (note medical and social transition don’t necessarily resolve gender dysphoria, and both may be followed by destransition). This is from the Cass Review commissioned by the UK National Health Services (page 57, Interim Report):

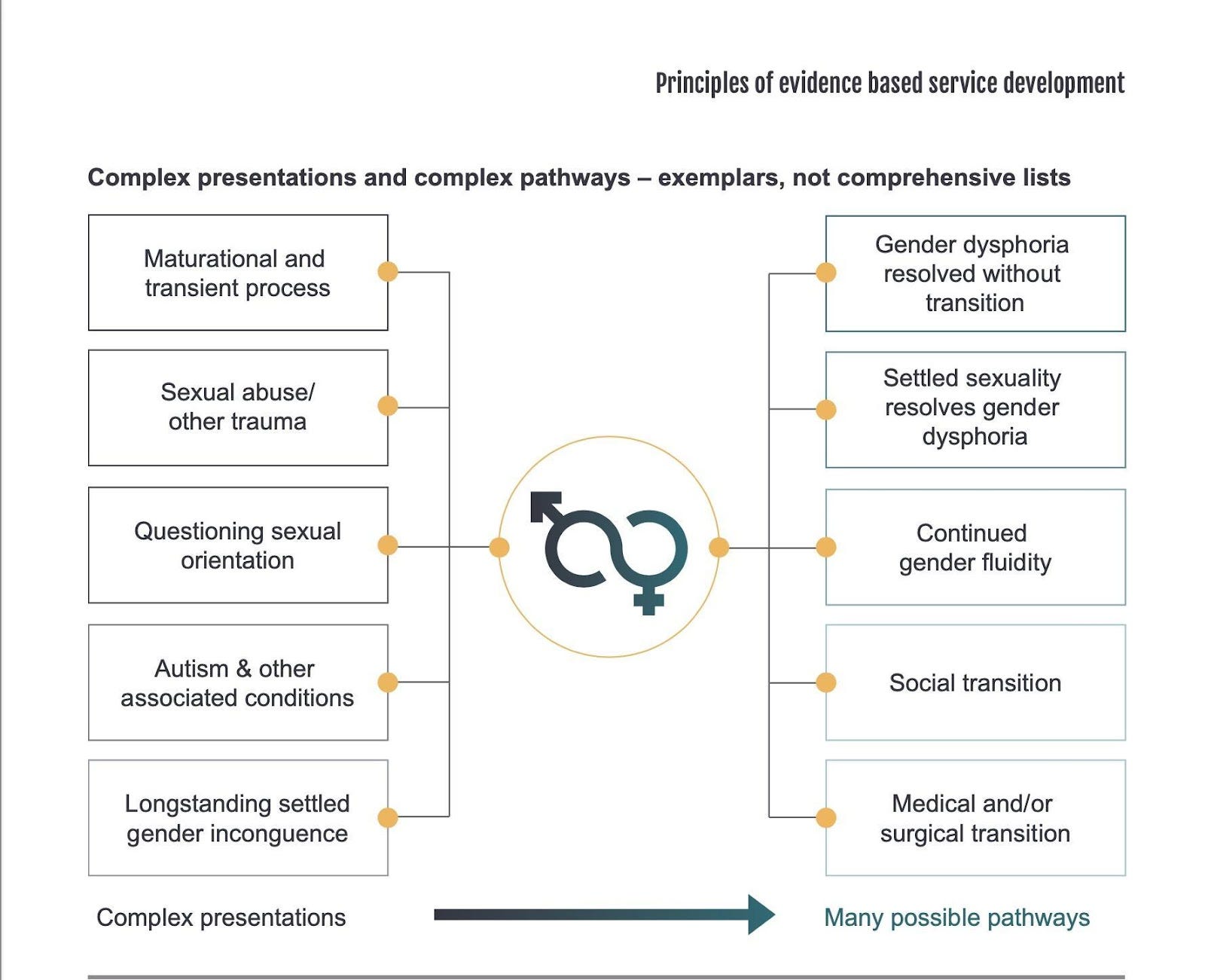{kind=link}
Why is there so much disagreement and uncertainty around treatment? In short, because the evidence is inadequate.[4] Formally, systematic evidence reviews can help sort out disagreements in the literature by finding out what studies have been done and grading how reliable they are in predicting outcomes. For gender dysphoria and its treatments, the answer is “unreliable”. That is, systematic reviews find the evidence behind medical interventions is low and very low quality– the studies cannot be used to reliably estimate outcomes. An overview of systematic reviews led by a world expert in systematic evidence review found the same.
Based upon its systematic review for minors, Sweden determined that the risks of puberty blockers and hormones in general outweigh the benefits (they then proposed only allowing medical intervention for minors in exceptional cases, and only in studies). The French National Academy of Medicine now recommends prioritizing psychotherapy for gender dysphoria, due to concerns of social influence and the inability to tell when transgender identification isn’t transient (note that even for non-transient gender dysphoria medical intervention has not been shown to be reliably beneficial). After their own review, Finland now recommends psychotherapy as first line, and restricts medical intervention below age 25. Similarly, Norway has just characterized medical intervention for young people as “treatments under trial.” The UK central clinic for children and adolescents is closing soon in part because practitioners were feeling pressured to offer unquestioning affirmation (common in the US) rather than holistically exploring underlying issues, exploration which sometimes finds medical intervention is not appropriate. A UK investigative reporter’s findings are just coming out and people are rightly horrified.
I strongly believe American trans identified kids deserve supportive care which protects them from medical harm as well.
When a trans identity is temporary or when medical intervention is otherwise inappropriate, medical intervention is iatrogenic (medically induced) harm, not “care.” These are serious, often irreversible, interventions: interruption of puberty with unclear consequences, overload of hormones (to amounts characteristic of disease), surgical removal of healthy body parts, removal or atrophy of necessary parts of the endocrine and reproductive system–and of course fertility is at risk. Over the long term, interventions are associated with serious heart and other cardiovascular damage, immune disease, bone harm, shortened life expectancy and more.
Even the doctors don’t know(!)[5] how many young people have been harmed by inappropriate medical intervention or have detransitioned. I find this astounding. Doctors don’t know how many of their patients regret having double mastectomies, sterility or their genitals removed, because they are not following them into the future. There are anecdotes but no statistics. I’m sure you’ve seen several people who are happy long term, but how many are like them? We don’t know. (Long-term has to be long enough. Poor outcomes and regret have been seen to surface between 3–6-8–10 years on average or as a median, depending upon study, sex, criteria for medical intervention, and the particular intervention.) And similarly, the detransitioners and regretters speaking out publicly are certainly not the only ones there are. Shame can contribute to gender dysphoria arising in the first place, and sometimes continues to be present, and detransitioning itself can be met with rejection and even abuse. Publicly stating that transition was a mistake and is regretted takes an enormous amount of courage. We just do not know how many detransitioners there are.
Here in the US, FDA approval has not been given for any drugs for treating gender dysphoria at any age, meaning benefit has not been shown to outweigh risk (the FDA oversees medications in the US). This is consistent with what Sweden and other countries have found. I had thought that someone feeling gender dysphoria would go to a clinic where they would be carefully evaluated in order to determine what would best help them, using what was known about how gender dysphoria can develop and what approaches work best for whom. However, as far as careful evaluation goes, US pediatric clinics tend to follow the new[6] US affirmation-only model, where medical intervention can even be offered on the first clinic visit. The affirmative approach was recommended as policy in 2018 by the American Academy of Pediatrics, but it (and the medical society guidelines it appeals to) rest on shaky ground: a peer-reviewed paper quickly showed[7] that the policy authors misrepresented studies to justify adopting affirmation. (Many AAP members have been trying, so far unsuccessfully, to get the AAP to do its own systematic review as part of their upcoming 2023 policy revision.) For young people over 18, affirmative “care” includes availability of medical interventions online and “informed consent”, where medical intervention does not require mental health evaluation. Not surprisingly, young people are often very far from being accurately informed. It does not help that many clinicians are poorly informed as well.
Although the research evidence cannot establish that indiscriminately medicalizing young people with this flawed “affirmation only” model is more beneficial than harmful, over 17,000 minors in the US were started on puberty blockers and hormones in 2017-2021. This is happening right here in the US, in spite of the abovementioned disagreement among experts, the lack of information about long-term outcomes, and the inability to determine when gender dysphoria will persist even after time or therapy. And just recently, reminiscent of the breaking UK scandal, a US university pediatric clinic’s shocking approach was detailed by Jamie Reed, a case worker with an MS in clinical research management, in her recent sworn affidavit and interview. Where are the studies showing that these treatments are safe and effective?[8] Several clinicians are asking why these treatments are being offered so broadly, and outside of experimental contexts, given the current failure of evidence to show they will help and outcomes showing significant harm.
How to help
If you want to support these young people, please join the many doctors, parents, trans people, detransitioners, and many others[9] who have been trying to get them appropriate evidence-based care–care that takes into account the different ways gender dysphoria occurs and resolves, as well as the fact that much is still unknown. Other countries are already doing so. The US is not following the science, and the harm to young people is accumulating rapidly. Please call for the lack of evidence to be remedied, for medical intervention only in carefully supervised clinical trials until more is known (these interventions involve irreversible physical changes, including risks to future fertility and sexual function, a fundamental human right), and for supportive therapy to help people figure out where their gender dysphoria is coming from, in case it is treatable non-invasively. Please join us in calling for and showing respect, celebration and love for all of them!
And thank you for reading all the way through. I hope that together we can help bring sanity, empathy and science back into this terribly fraught situation for young people.
[1] Opening an umbrella is associated with rain but will not cause rain to fall–the usual “correlation is not causation” fallacy. The above quoted paper had this problem and others called out here (Biggs, 2020; this paper also referenced below for suicide claims).
[2] No, this isn’t like lefthandedness, which rose only by a factor of about 6 and took about 40 years to do so (and was rising roughly back to its earlier rate).
[3] Trans is not the new gay—being gay is determined by who you are attracted to sexually, not how you see yourself. Being trans-identified is a belief about one’s self. Beliefs about oneself can change over time.
[4] In addition, a lot of incorrect information is circulating. Here is (a video of) expert testimony by Dr. Stephen Levine, spelling some of it out.
[5] Quoted numbers from studies are usually flawed, measuring outcomes too soon, not tracking everyone, measuring something inappropriate or the wrong sample. Although one might be told that <1% who have surgery regret it; to be counted as a regretter in that study, you had to reverse the hormones you asked for and mention regret in a clinic visit. Of the patients, 36% stopped coming in for lifetime treatment, and weren’t followed up–it’s unclear how many of that 36% stopped for good or regretted (if you regretted, stopping would be appropriate). Another study found that almost 30% of those taking lifetime hormones stopped after 4 years. Results for rates also depend on who is included in the study. Regret numbers are completely unknown.
[6] Only about a decade old
[7] From the peer reviewed expert critique: “Although almost all clinics and professional associations in the world use what’s called the watchful waiting approach to helping gender diverse (GD) children, the AAP statement rejected that consensus, endorsing gender affirmation as the only acceptable approach. Remarkably, not only did the AAP statement fail to include any of the actual literature on outcomes on such cases, but it also misrepresented the contents of its citations, which repeatedly said the very opposite of what AAP attributed to them.”
[8] There are several well-advertised studies and compilations that demonstrate a lot less than one realizes at first glance, given some (inaccurate) headlines. A pile of studies claiming something is true is not enough if the studies are poorly done, are not representative, don’t wait long enough to measure outcomes, and/or lose participants… that’s why evidence based medicine is important (formal rebuttals are too, e.g., here, here, here, here, and in links above, but take time to write and publish, and unfortunately there is a lot needing correction).
[9] Some of many places to learn more: other Genspect essays, Pitt (parent stories), Broadview (Lisa Selin Davis), Gender Clinic News (Bernard Lane in Australia), Society for Evidence-Based Gender Medicine (research updates and policy updates), Gender: A wider lens (weekly podcast with a wide range of interviews), for parents also Stella O’Malley’s substack and Sasha Ayad’s pages….there is much, much more beyond these, as well.