
ABSTRACT
This policy statement from Genspect calls for restoring psychiatric safeguards in the treatment of gender-related distress through the re-psychopathologization of the drive to medically transition. Using the clinical construct of the extreme overvalued belief, it identifies the obsessive pursuit of irreversible body modification as a pathological fixation rather than an innate identity. Genspect argues that WPATH’s de-psychopathologization campaign was politically motivated and thereby removed essential mental health protections and enabled medical overreach. Evidence of poor long-term outcomes and rising harm supports the need to re-establish psychiatric frameworks, end affirmation-only protocols, and protect minors and vulnerable adults. Restoring a therapeutic model grounded in psychiatry is both a clinical and ethical imperative.
EXECUTIVE SUMMARY
Genspect calls for the restoration of mental health safeguards in the treatment of gender-related distress through our campaign to re-psychopathologize the drive to medically transition. We seek to restore clinical understanding within a coherent psychiatric framework, distinguishing pathological fixation from the broader and often transient experiences of gender questioning or nonconformity.
WPATH’s 2010 de-psychopathologization campaign was an act of political advocacy rather than scientific discovery. It systematically dismantled psychiatric safeguards by declaring transgender identity innate and healthy (2010), demoting mental health professionals to facilitators in Standards of Care 7 (2012), replacing Gender Identity Disorder with Gender Dysphoria in the DSM-5 (2013) and with Gender Incongruence in the ICD-11 (2018), redefining medical transition as medically necessary (2016), and removing age barriers in Standards of Care 8 (2022).
These changes coincided with a sharp rise in medical transition, more regret and detransition, and a social contagion pattern among youth, especially adolescent girls. Our review of the literature and clinical consultations indicate that the obsessive pursuit of radical, permanent body modification including surgery and cross-sex hormones represents a pathological condition that requires therapy, not affirmation.
For this reason, we have initiated a counter-campaign to re-psychopathologize the drive to medically transition.
The concept of the extreme overvalued belief provides a coherent clinical framework for understanding this phenomenon. Coined in 2019 by psychiatrist Tahir Rahman, the term describes beliefs that are rigid and all-consuming, but non-delusional because they are shared by others in a culture or subculture. Rahman drew on the well-established psychiatric concept of an overvalued idea, first described by psychiatrist Carl Wernicke in 1892. To the holder they feel rational and even noble, and are defended with passionate certainty. Cultural validation is central to their spread. Rahman and colleagues emphasize the relevance of this concept to contemporary psychiatry, particularly in explaining how culturally reinforced convictions can drive harmful behavior (Rahman et al., 2019; Rahman et al., 2020; Rahman & Abugel, 2024).
This belief system now shapes parts of the medical establishment. Many patients encounter professionals influenced by the same conviction, which channels distress toward irreversible interventions rather than therapeutic exploration. Vulnerable individuals seeking help often encounter professionals who are influenced by the same overvalued belief, reinforcing the assumption that an individual’s self-perception as transgender is healthy and should lead to irreversible medical interventions rather than therapeutic exploration and recovery.
This phenomenon mirrors another episode in psychiatry’s recent history where an extreme overvalued belief eclipsed clinical judgment. The recovered memory and multiple personality disorder movements of the 1980s and 1990s represent clear examples of extreme overvalued beliefs, in which suggestive therapeutic practices gave rise to widespread false memories and moral panic, tearing families apart (McHugh, 2008).
While the lobotomy era of the mid-twentieth century did not reflect an extreme overvalued belief, it illustrates another recurrent danger within psychiatry and medicine, where professional overreach was driven by misplaced confidence in radical intervention. Tens of thousands of patients were permanently harmed by a procedure once promoted as both compassionate and progressive (Mashour et al., 2005; Raz, 2013; El-Hai, 2005).
The current crisis in so-called “gender medicine” combines both patterns, as ideological conviction displaces clinical objectivity and medical overreach masquerades as care, drawing vulnerable individuals into a belief system that presents itself as benevolent but functions as pathology.
Outcomes undermine claims of benefit. Studies report elevated rates of depression, unemployment, psychiatric hospitalization, incarceration, and suicide after medical transition (Bränström & Pachankis, 2020; Dhejne et al., 2011; Kohnepoushi et al., 2023; Lam et al., 2022; Van de Cauter et al., 2021; Wiepjes et al., 2020). Adolescents are being fast-tracked to irreversible procedures, and detransitioners report lasting physical and psychological harm (Cohn, 2023; Littman et al., 2024; Roberts et al., 2022). Families are also left devastated, bearing the consequences of a system that mistook affirmation for care.
We urge governments, medical associations, and mental health bodies to recognize this as a pathological condition characterized by an extreme overvalued belief, reverse WPATH-based policies, restore psychiatric frameworks that enable appropriate therapeutic intervention, and end affirmation-only protocols. Medical standards must once again recognize this condition as a mental disorder requiring psychosocial treatment, and children, adolescents, and vulnerable adults must be protected from experimental interventions driven by social contagion and reinforced by medical collusion with pathological belief.
This should not be mistaken for stigmatization. It represents the restoration of clinical clarity. As psychiatrist Allen Frances (2013) has observed, a diagnosis is only justified if it benefits the patient by guiding effective treatment and improving outcomes. Recognizing the pathological drive toward medical transition allows clinicians to meet this standard and provide meaningful therapeutic care. Clinicians require a shared clinical construct to identify and treat this presentation. In every area of psychiatry, well-defined frameworks provide the common language and diagnostic thresholds necessary for consistent assessment, risk communication, and intervention. The extreme overvalued belief framework fulfills this role for cases of pathological fixation on medical transition. This document supplies the terminology, criteria, and clinical guidance needed to ensure safe and effective care.
I. THE PROBLEM
The following section provides the clinical and evidentiary foundation for the concerns outlined in the Executive Summary. It expands on the underlying psychopathology, the structural causes of its institutionalization within “gender medicine,” and the mechanisms through which cultural reinforcement has transformed a psychiatric condition into a purportedly healthy identity that demands drastic medical interventions.
A. The Clinical Threshold
This policy addresses a specific pathological condition, not gender nonconformity or identity exploration. The pathology emerges when an individual crosses a definable clinical threshold characterized by:
- Developing a fixed conviction that medical transition is necessary and inherently beneficial
- Viewing the body as fundamentally wrong and requiring surgical or hormonal alteration
- Allowing this conviction to overtake the individual’s sense of self, becoming the central organizing principle of identity
- Experiencing this belief as entirely rational and even noble, and defending it with passionate intensity resistant to challenge
- Reinforcing and amplifying this conviction within subcultures or online communities that celebrate transition as liberation
- Exhibiting significant loss of flexibility, preoccupation that crowds out other life goals, minimization of risk, and rejection of alternative explanations or therapeutic approaches
- Demonstrating functional impairment or self-destructive behavior resulting from the fixation
This constellation defines an extreme overvalued belief that drives pathological behavior, specifically self-directed harm against healthy body parts.
This policy does not classify all trans-identifying individuals as having an extreme overvalued belief. The framework applies only when three features occur together. First, a fixed conviction that body modification is necessary and inherently beneficial. Second, significant rigidity that resists alternative explanations or therapeutic goals. Third, an all-consuming and self-destructive pursuit of irreversible medical interventions despite clear risks and unresolved psychological issues. When identity exploration is flexible, distress is proportionate, and individuals are open to therapy, supportive care and standard differential assessment are appropriate rather than an extreme overvalued belief formulation.
B. How WPATH’s De-Psychopathologization Created This Crisis
WPATH’s de-psychopathologization campaign constructed a logical framework that made medical transition appear inevitable while systematically dismantling clinical safeguards.
The Constructed Logic
- Premise 1 – Transgender identity is innate, healthy, and normal (WPATH, 2010).
- Premise 2 – If the identity is healthy, the problem cannot reside in the identity itself.
- Premise 3 – Therefore, the problem must lie in the body’s failure to match that identity.
- Conclusion – Medical body modification becomes the logical solution and is labeled medically necessary (WPATH, 2016).
- Corollary – Therapeutic attempts to address the identity are redefined as conversion therapy.
Systematic Implementation
- 2010 – WPATH declared transgender identity innate, healthy, and to be celebrated (WPATH, 2010).
- 2012 – WPATH Standards of Care Version 7 demoted mental health professionals from providing a meaningful therapeutic process to serving as facilitators of medical transition (Coleman et al., 2012).
- 2013 – The DSM-5 replaced Gender Identity Disorder—which treated the cross-sex identity itself as pathological—with Gender Dysphoria, which framed the identity as healthy and the distress as the pathology. This redefinition removed any framework for addressing underlying psychological causes. It also explained that a person’s “strong desire to be rid of their secondary sex characteristics” stemmed from “a marked incongruence with their experienced gender” (APA, 2013)—in other words, treatment begins with the assumption that the person is transgender.
- 2016 – WPATH defined medical transition as medically necessary and advocated for insurance coverage (WPATH, 2016).
- 2018 – The World Health Organization’s ICD-11 reclassified Gender Identity Disorder as Gender Incongruence, moving it out of the chapter on mental disorders and into Conditions Related to Sexual Health (World Health Organization, 2018).
- 2022 – WPATH Standards of Care Version 8 removed age barriers for radical and irreversible interventions, including mastectomies and cross-sex hormones (Coleman et al., 2022).
C. The Dual Pathology
In the field of gender medicine today, the danger is profoundly amplified because the extreme overvalued belief has influenced both vulnerable individuals and the medical establishment. WPATH and its affiliated practitioners now operate within an echo chamber devoid of ideological diversity, open debate, or critical self-reflection. Vulnerable individuals seeking help often encounter professionals who share and reinforce the same overvalued belief, leading to affirmation and acceleration toward irreversible interventions rather than appropriate therapeutic care.
This dynamic reflects a recurring pattern in psychiatric history, where ideological certainty displaces clinical judgment and produces harmful consequences for patients and families.
The recovered memory movement of the 1980s and 1990s provides a perfect parallel to demonstrate psychiatry’s capacity to become swept up by harmful false beliefs. Recovered memory enthusiasts believed in the pseudoscientific notion of repressed memories of childhood sexual abuse that could be recovered through specific techniques involving hypnosis, suggestion, and often barbiturates. The mental health professionals influenced by this extreme overvalued belief created an epidemic of false allegations of child sex abuse that destroyed families (Loftus & Ketcham, 1994; McHugh, 2008; McNally, 2003). The certainty with which practitioners defended their methods—despite mounting evidence of suggestion-induced false memories—mirrors contemporary resistance to evidence that challenges affirmative care protocols. Those same recovered memory enthusiasts triggered the related multiple personality disorder (MPD) epidemic, using the same techniques but flavored with the belief that repressing memories of abuse caused the personality to fracture as a coping mechanism. The resulting MPD subculture of specialized clinicians operated as a closed system that interpreted skepticism as denial of patient suffering (McHugh, 2008; Piper & Merskey, 2004).
The lobotomy era, driven more by institutional momentum than ideological conviction, illustrates how medical enthusiasm for drastic life-altering procedures can outpace evidence. Physicians promoted a radical and irreversible procedure despite minimal proof of benefit, presenting it as both progressive and compassionate. Only decades later was the catastrophic harm fully acknowledged, after tens of thousands had been permanently damaged (El-Hai, 2005; Mashour et al., 2005; Raz, 2013).
These episodes share a common structure: ideological certainty or professional overreach displacing evidence-based practice, institutional systems that reinforce rather than correct error, vulnerable patients subjected to irreversible interventions, and systemic resistance to acknowledging harm until it becomes undeniable.
II. THE EVIDENCE
A. Clinical Framework
The following section outlines the clinical framework necessary to understand gender-related pathology through the lens of extreme overvalued beliefs. The concept of the overvalued idea was first introduced by psychiatrist Carl Wernicke in 1892 and has remained a recognized construct in psychiatry for more than a century (Wernicke, 1892). It was later refined by Rahman and colleagues, who redefined it as an extreme overvalued belief and emphasized its relevance to contemporary psychiatry, particularly in explaining how culturally reinforced convictions can drive harmful behavior (Rahman et al., 2019).
An extreme overvalued belief is a rigid, non-delusional conviction that differs from both a delusion (a psychotic detachment from reality) and an obsession (an intrusive, distressing thought). It is characterized by:
- Overtaking the individual’s entire sense of self
- Being experienced as entirely rational and often noble
- Being shared and reinforced within subcultures or echo chambers
- Being defended with passionate and inflexible intensity
- Driving powerful actions, including self-destructive or violent behavior
- Causing little or no distress in itself, with distress arising primarily from obstacles to acting upon it
Critical recognition – Cultural and social reinforcement are not separate from this pathology but central to its function (Rahman et al., 2019). Extreme overvalued beliefs require cultural validation in order to persist and intensify. Recognizing social contagion dynamics does not contradict psychopathologization; it clarifies the mechanism through which this pathology spreads.
B. Outcome Data
If the drive to medically transition were healthy, we would expect to see sustained improvements in mental health and psychosocial outcomes. Objective evidence demonstrates the opposite. Across multiple studies and national datasets, individuals who undergo medical transition exhibit significantly elevated rates of:
- Depression (Bränström & Pachankis, 2020; Dhejne et al., 2011)
- Unemployment (Van de Cauter et al., 2021; Van de Cauter et al., 2024)
- Psychiatric hospitalization (Dhejne et al., 2011; Lam et al., 2022)
- Incarceration (Dhejne et al., 2011)
- Death by suicide (Dhejne et al., 2011; Kohnepoushi et al., 2023; Wiepjes et al., 2020)
These findings indicate that medical transition does not resolve underlying distress but instead represents a pathological response to a pathological fixation. The procedures involved—surgical removal of healthy tissue, construction of non-functional pseudo-genitalia, and chemical disruption of the endocrine system—constitute forms of self-directed harm, facilitated by medical professionals who have misinterpreted pathology as identity. What these individuals needed was recognition of their compulsive drive (in natal males, sometimes driven by paraphilic interests such as autogynephilia that escalate to pursuit of surgical modification; Blanchard, 1989) and access to appropriate therapeutic intervention, not affirmation that hastened irreversible damage.
C. Documented Harm
Vulnerable individuals—particularly adolescents caught in patterns of social contagion—are being fast-tracked toward irreversible medical interventions (Cass, 2024; Kaltiala et al., 2020; Levine et al., 2022). Detransitioners are left with permanent physical and psychological harm (Butler & Hutchinson, 2020; Cohn, 2023; Littman et al., 2024; Roberts et al., 2022). Families have been fractured, and lives have been irreparably altered by a system that celebrates a pathological fixation instead of addressing the underlying condition.
The largest prospective studies on puberty blockers—conducted by Dr. Polly Carmichael in the United Kingdom and Dr. Johanna Olson-Kennedy in the United States—found no significant psychological improvement from these interventions. Carmichael et al. (2021) followed 44 young people aged 12 to 15 on puberty blockers and reported no changes in psychological functioning or self-harm scores, with 98% proceeding to cross-sex hormones. Similarly, Olson-Kennedy et al. (2025) found no significant change in depression symptoms over 24 months of puberty blocker treatment in 94 participants. Both studies were delayed for approximately ten years before publication, raising serious concerns about research transparency in pediatric “gender medicine.”
Medical transition carries serious, documented harms across surgical and hormonal pathways, with long-term safety remaining uncertain. In a Swedish population cohort, people who underwent sex-reassignment surgery later showed sharply worse outcomes than the general population: 19-fold higher suicide mortality, 2.8× higher overall mortality, 4.9× higher suicide-attempt rates, and 2.8× higher psychiatric-hospitalization rates (Dhejne et al., 2011). Surgical complications are frequent and clinically significant: phalloplasty shows a 76.5% overall complication rate with 34% developing urethral fistulas (Wang et al., 2022); vaginoplasty produces urinary complications in ~5–12% depending on type, with meatal stenosis averaging 6.9% across studies and reaching 40% in one series using older techniques (Ding et al., 2022; Manrique et al., 2018; Nassiri et al., 2021). Oophorectomies surgically induce menopause in healthy young women, dramatically increasing the risk of heart disease, stroke, osteoporosis and early death (Rocca et al., 2006). The cardiovascular risks of surgical menopause are well established and far greater than those of natural menopause (van der Schouw et al., 1996). Cross-sex hormones also carry cardiovascular and metabolic risks—estrogen in males is linked to a 9.9-fold increase in ischemic stroke after six years and a 5.5-fold increase in venous thromboembolism (Getahun et al., 2018; Nota et al., 2019), while testosterone in females is associated with rises in blood pressure, BMI, and adverse lipid profiles—yet the UK’s National Institute for Health and Care Excellence rated the overall evidence base as “very low certainty” and emphasized that any perceived benefits must be weighed against a largely unknown long-term safety profile (National Institute for Health and Care Excellence, 2020).
Vulnerable populations face compounded risks. Children and adolescents with autism spectrum disorder are markedly overrepresented in gender clinics, with prevalence estimates ranging from 11% to as high as 68% in some samples (Kallitsounaki & Williams, 2022; Shumer et al., 2016; Warrier et al., 2020). Same-sex attraction is also markedly over-represented, with 2015 data from the UK’s Gender Identity Development Service showing rates of approximately 60% among boys and 70% among girls (Gender Identity Development Service, n.d.). Youth with gender dysphoria show 3.72 times greater odds of an eating disorder diagnosis, with co-occurring conditions linked to significantly higher rates of anxiety, depression, suicidality, and self-harm (Abernathey et al., 2024).
Social contagion dynamics have been documented in cases of rapid-onset gender dysphoria, where distress emerges suddenly during or after puberty without childhood indicators. This presentation predominantly affects natal females and is frequently associated with pre-existing mental health conditions and patterns of peer influence (Littman, 2018).
These harms are not incidental but systemic, arising from cultural and institutional frameworks that reinforce the underlying pathology rather than resolve it. The following section outlines how this mechanism of reinforcement operates and identifies the measures required to restore clinical integrity.
III. RE-PSYCHOPATHOLOGIZATION: REQUIREMENTS AND RATIONALE
A. Definition and Scope
Psychopathologization is used here in its conventional clinical sense—the recognition and conceptualization of a condition as a mental disorder requiring psychiatric, psychological, or psychotherapeutic support. It re-establishes a coherent clinical framework for understanding behavior that has been ideologically misinterpreted as identity. This framing is clinically neutral and essential for effective care. To deny that an individual suffers from a mental disorder when the evidence clearly demonstrates otherwise is not an act of compassion; it is a denial of access to appropriate treatment.
Re-psychopathologization therefore restores clinical integrity and re-establishes the capacity to provide appropriate help to individuals consumed by a harmful fixation that drives them toward irreversible bodily harm.
B. Clinical Requirements
Re-psychopathologization requires the restoration of sound psychiatric principles and recognition that, in many cases, trans identification functions as a maladaptive coping mechanism for psychological distress. When reinforced, this mechanism may progress into pathological behavior, resulting in self-directed harm and long-term medical dependency.
Clinical recognition: The pathological drive to medically transition must be recognized as an all-consuming fixation that leads to self-destructive behavior, not as an innate identity requiring medical accommodation. Trans identification can function as a maladaptive coping response to issues such as trauma, anxiety, depression, social alienation, or identity confusion. Proper clinical recognition entails identifying the psychological conflicts and developmental vulnerabilities that fuel this fixation and addressing these root causes through a meaningful therapeutic process rather than enabling the compulsive pursuit of body modification.
Therapeutic intervention: Comprehensive psychological treatment should directly address the extreme overvalued belief itself. Therapy should introduce essential countervailing perspectives and help individuals understand how the fixation developed, why it fails to alleviate distress, and how pursuing it will cause permanent physical harm. Treatment may focus on strengthening ego function, developing distress tolerance, and building alternative coping strategies that do not involve medical self-destruction. The therapeutic aim is psychological integration of the self, not alignment with a delusional ideal of transformation.
Safeguarding and Escalation
- Moderate risk: persistent fixation with emerging impairment → structured outpatient therapy; family engagement; reduce exposure to reinforcing contexts; scheduled re-evaluation.
- High risk: acute self-harm risk, rapid deterioration, or coercive reinforcement → urgent psychiatric assessment; consider higher level of care.
- Minors: defer irreversible interventions; require multidisciplinary case review, parental/guardian involvement, and periodic re-evaluation at defined intervals.
Cessation of Reinforcement: Institutional and cultural systems must cease validating and amplifying this pathology. Schools, clinics, healthcare systems, mental health organizations, and social media platforms currently act as reinforcing agents of the maladaptive belief, providing social validation rather than therapeutic containment. Affirmation-only protocols must end, as they entrench the fixation rather than resolve it. Subcultures that celebrate transition as liberation should be understood to function as pathological echo chambers that trap individuals in cycles of self-harm and social isolation.
Restoration of Clinical Authority: Mental health professionals should be empowered to treat the underlying pathology rather than act as facilitators of medical transition. Clinical authority has been eroded by ideological pressure, leaving practitioners afraid to explore the psychological origins of gender distress. Restoring professional autonomy means reaffirming the clinician’s duty to do no harm, to question the patient’s beliefs compassionately, and to guide them toward psychological healing rather than body modification and medical dependence.
Professional Independence: Medical standards must be re-established outside the WPATH echo chamber by clinicians free from the same overvalued belief that has captured the field. Professional independence requires separating scientific medicine from ideological activism and ensuring that diagnostic and treatment frameworks are guided by empirical evidence, not political dogma. Independent oversight bodies must be formed to review current practices and ensure ethical accountability within gender medicine.
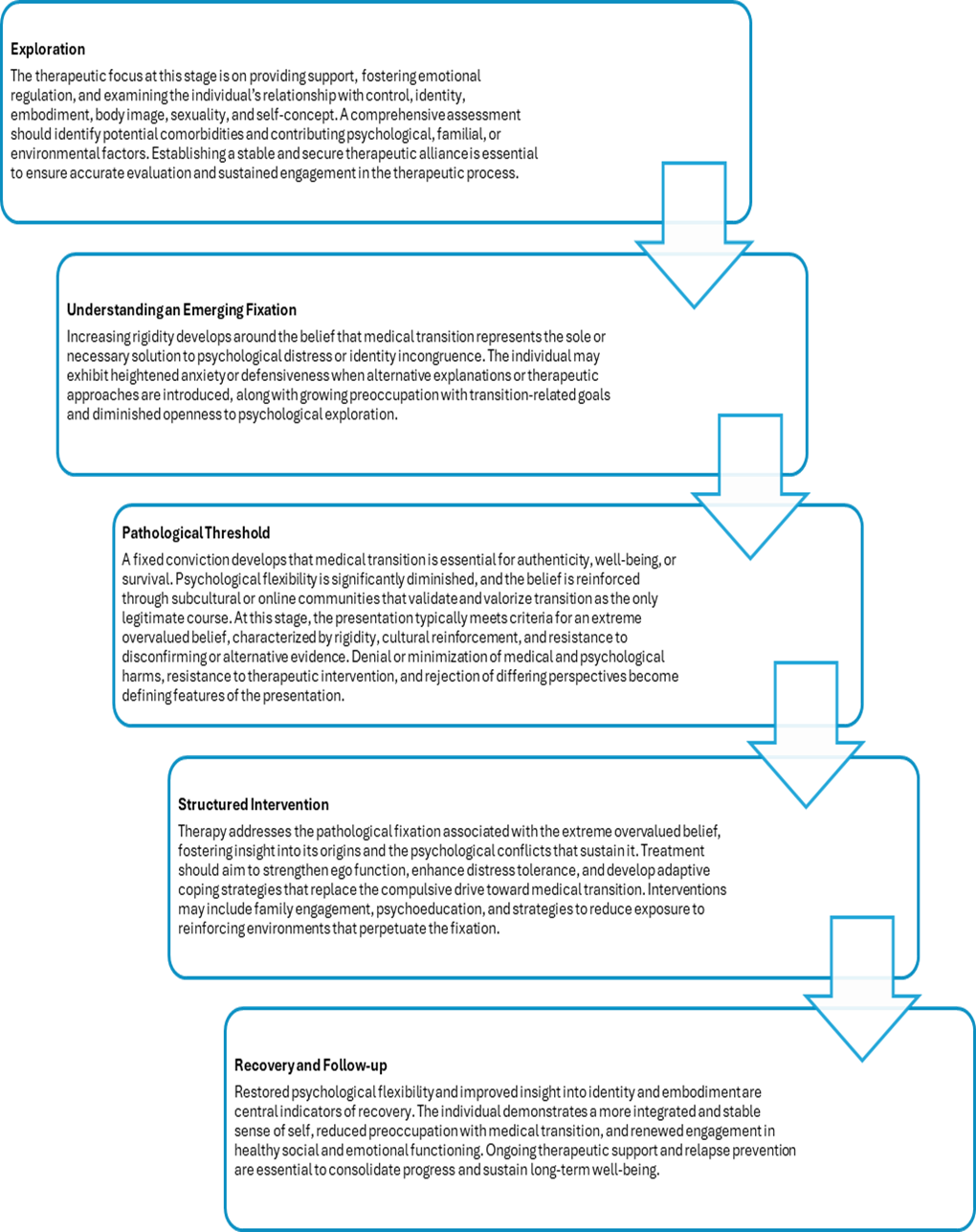
Figure 1. Clinical Formulation of Pathological Fixation on Medical Transition
IV. CALL TO ACTION
Genspect calls upon governments, medical associations, and mental health authorities to take immediate and coordinated action to restore clinical integrity in the treatment of gender-related distress. Specifically, we urge the following actions.
Recognition: Acknowledge that the compulsive drive toward medical transition constitutes a pathological condition characterized by an extreme overvalued belief and recognize that cultural and social reinforcement mechanisms are central to how this pathology develops and spreads.
Policy reversal: Rescind all policies derived from WPATH’s de-psychopathologization campaign, which established a direct pathway from self-identified gender identity to irreversible medical intervention.
Restoration of psychiatric care: Reinstate psychiatric and psychological frameworks for treating this as a serious mental health condition requiring therapeutic intervention to address the underlying pathology.
Termination of affirmation-only protocols: End clinical practices that reinforce the extreme overvalued belief and accelerate vulnerable individuals toward irreversible surgical and hormonal procedures.
Independent medical standards: Recognize that many practitioners engaged in so-called gender-affirming care have internalized the same overvalued belief affecting their patients and establish medical standards and oversight bodies independent of WPATH and similar ideological frameworks.
Protection of vulnerable populations: Safeguard children, adolescents, and vulnerable adults from experimental medical interventions driven by social contagion, cultural reinforcement, and institutional collusion with pathological belief systems.
Integration of social contagion research: Incorporate research on social contagion and cultural reinforcement dynamics as essential to understanding and interrupting the spread of this pathology.
V. CONCLUSION
WPATH’s de-psychopathologization campaign was an act of ideological advocacy that dismantled essential psychiatric safeguards, removed the capacity to treat an underlying pathological condition, and created a direct pathway from identity confusion to irreversible medical harm inflicted on healthy bodies.
The result has been catastrophic. Vulnerable individuals—particularly adolescents caught in social contagion dynamics and cultural echo chambers—are being fast-tracked toward permanent body modification by a medical establishment influenced by the same pathological fixation.
This re-psychopathologization campaign is grounded in psychiatric principles that have been recognized for over a century, from Wernicke’s original formulation to contemporary understanding of how extreme beliefs drive harmful behavior. It is motivated by clinical truth and by what is now undeniable: devastated families, harmed detransitioners, and vulnerable people whose lives have been destroyed by a system that celebrated their fixation rather than treated their condition.
This is not an act of stigmatization but a necessary restoration of clinical clarity and ethical responsibility. Only by recognizing the pathological drive toward medical transition and understanding how it is sustained through cultural reinforcement can the medical and mental health professions recover their integrity, protect the vulnerable, and rebuild public trust. Genspect calls for courage, compassion, and intellectual honesty to confront this crisis and ensure that therapeutic care—not ideological affirmation—defines the future of safe and ethical treatment for this vulnerable cohort of patients. Restoring a therapeutic model is not merely an academic correction—it is an act of compassion toward those misled into self-harm by a culture that mistook distress for identity.
REFERENCES
Abernathey, L., Kahn, N. F., Sequeira, G. M., Richardson, L. P., & Ahrens, K. (2024). Associations between gender dysphoria, eating disorders, and mental health diagnoses among adolescents. Journal of Adolescent Health, 75(5), 780-784. https://doi.org/10.1016/j.jadohealth.2024.06.022
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425596
Blanchard, R. (1989). The concept of autogynephilia and the typology of male gender dysphoria. Journal of Nervous and Mental Disease, 177(10), 616–623. https://doi.org/10.1097/00005053-198910000-00004
Bränström, R., & Pachankis, J. E. (2020). Reduction in mental health treatment utilization among transgender individuals after gender-affirming surgeries: A total population study. American Journal of Psychiatry, 177(8), 727–734. https://doi.org/10.1176/appi.ajp.2019.19010080
Butler, C., & Hutchinson, A. (2020). Debate: The pressing need for research and services for gender desisters/detransitioners. Child and Adolescent Mental Health, 25(1), 45–47. https://doi.org/10.1111/camh.12361
Carmichael, P., Butler, G., Masic, U., Cole, T. J., De Stavola, B. L., Davidson, S., Skageberg, E. M., Khadr, S., & Viner, R. M. (2021). Short-term outcomes of pubertal suppression in a selected cohort of 12- to 15-year-old young people with persistent gender dysphoria in the UK. PLOS ONE, 16(2), e0243894. https://doi.org/10.1371/journal.pone.0243894
Cass, H. (2024). Independent review of gender identity services for children and young people: Final report. NHS England. https://cass.independent-review.uk/home/publications/final-report/
Cohn, J. (2023). The detransition rate is unknown. Archives of Sexual Behavior, 52(5), 1937-1952. https://doi.org/10.1007/s10508-023-02623-5
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L. C., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F. L., Monstrey, S. J., Motmans, J., Nahata, L., … Winter, S. (2012). Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. International Journal of Transgenderism, 13(4), 165–232. https://doi.org/10.1080/15532739.2011.700873
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L. C., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F. L., Monstrey, S. J., Motmans, J., Nahata, L., … Winter, S. (2022). Standards of care for the health of transgender and gender diverse people, version 8. International Journal of Transgender Health, 23(Suppl. 1), S1–S259. https://doi.org/10.1080/26895269.2022.2100644
Dhejne, C., Lichtenstein, P., Boman, M., Johansson, A. L. V., Långström, N., & Landén, M. (2011). Long-term follow-up of transsexual persons undergoing sex reassignment surgery: Cohort study in Sweden. PLOS ONE, 6(2), e16885. https://doi.org/10.1371/journal.pone.0016885
Ding, C., Khondker, A., Goldenberg, M. G., Kwong, J. C. C., Lajkosz, K., Potter, E., Millman, A., Krakowsky, Y., & Perlis, N. (2022). Urinary complications after penile inversion vaginoplasty in transgender women: Systematic review and meta-analysis. Canadian Urological Association Journal, 17(4), 121-128. https://doi.org/10.5489/cuaj.8108
El-Hai, J. (2005). The lobotomist: A maverick medical genius and his tragic quest to rid the world of mental illness. Wiley. https://www.wiley.com/en-us/The+Lobotomist
Frances, A. (2013). Saving normal: An insider’s revolt against out-of-control psychiatric diagnosis, DSM-5, Big Pharma, and the medicalization of ordinary life. William Morrow. https://archive.org/details/savingnormalinsi0000fran
Gender Identity Development Service. (n.d.). Gender identity and sexuality. NHS. Retrieved January 31, 2024, from https://web.archive.org/web/20240131145148/https://gids.nhs.uk/gender-identity-and-sexuality/
Getahun, D., Nash, R., Flanders, W. D., Baxter, R., Becerra-Culqui, T. A., Cromwell, L., Hunkeler, E., Lash, T. L., Millman, A., Quinn, V. P., Robinson, B., Roblin, D., Silverberg, M. J., Slovis, J., Vin Tangpricha, Goodman, M., & Safer, J. (2018). Cross-sex hormones and acute cardiovascular events in transgender persons: A cohort study. Annals of Internal Medicine, 169(4), 205-213. https://doi.org/10.7326/M17-2785
Kallitsounaki, A., & Williams, D. M. (2022). Autism Spectrum Disorder and Gender Dysphoria/Incongruence. A systematic literature review and meta-analysis. Journal of Autism and Developmental Disorders, 53(8), 3103–3117. https://doi.org/10.1007/s10803-022-05517-y
Kaltiala, R., Bergman, H., Carmichael, P., de Graaf, N. M., Rischel, K. E., Frisén, L., Schorkopf, M., Suomalainen, L., & Waehre, A. (2020). Time trends in referrals to child and adolescent gender identity services: A study in four Nordic countries and in the UK. Nordic Journal of Psychiatry, 74(1), 40-44. https://doi.org/10.1080/08039488.2019.1667429
Kohnepoushi, P., Nikouei, M., Cheraghi, M., Hasanabadi, P., Rahmani, H., Moradi, M., Moradi, G., Moradpour, F., & Moradi, Y. (2023). Prevalence of suicidal thoughts and attempts in the transgender population of the world: A systematic review and meta-analysis. Annals of General Psychiatry, 22, Article 28. https://doi.org/10.1186/s12991-023-00460-3
Lam, J. S. H., Abramovich, A., Victor, J. C., Zaheer, J., & Kurdyak, P. (2022). Characteristics of transgender individuals with emergency department visits and hospitalizations for mental health. Psychiatric Services, 73(7), 722-729. https://doi.org/10.1176/appi.ps.202100306
Levine, S. B., Abbruzzese, E., & Mason, J. W. (2022). Reconsidering informed consent for trans-identified children, adolescents, and young adults. Journal of Sex & Marital Therapy, 48(7), 706–727. https://doi.org/10.1080/0092623X.2022.2046221
Littman, L. (2018). Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLOS ONE, 13(8), e0202330. https://doi.org/10.1371/journal.pone.0202330
Littman, L., O’Malley, S., Kerschner, H., & Bailey, J. M. (2024). Detransition and desistance among previously trans-identified young adults. Archives of Sexual Behavior, 53(1), 57-76. https://doi.org/10.1007/s10508-023-02716-1
Loftus, E. F., & Ketcham, K. (1994). The myth of repressed memory: False memories and allegations of sexual abuse. St. Martin’s Press. https://archive.org/details/mythofrepressedm00loft_0
Manrique, O. J., Adabi, K., Martinez-Jorge, J., Ciudad, P., Nicoli, F., & Kiranantawat, K. (2018). Complications and patient-reported outcomes in male-to-female vaginoplasty—Where we are today: A systematic review and meta-analysis. Annals of Plastic Surgery, 80(6), 684–691. https://doi.org/10.1097/SAP.0000000000001393
Mashour, G. A., Walker, E. E., & Martuza, R. L. (2005). Psychosurgery: Past, present, and future. Brain Research Reviews, 48(3), 409–419. https://doi.org/10.1016/j.brainresrev.2004.09.002
McHugh, P. R. (2008). Try to remember: Psychiatry’s clash over meaning, memory, and mind. Dana Press. https://books.google.com/books/about/Try_to_Remember.html?id=tipoNAAACAAJ
McNally, R. J. (2003). Remembering trauma. Harvard University Press. https://www.hup.harvard.edu/books/9780674018020
Nassiri, N., Maas, M., Basin, M., Cacciamani, G. E., & Doumanian, L. R. (2021). Urethral complications after gender reassignment surgery: A systematic review. International Journal of Impotence Research, 33(8), 793-800. https://doi.org/10.1038/s41443-020-0304-y
National Institute for Health and Care Excellence. (2020). Evidence review: Gender-affirming hormones for children and adolescents with gender dysphoria. NHS England. https://segm.org/sites/default/files/20210323_Evidence+review_Gender-affirming+hormones_For+upload_Final_download.pdf
Nota, N. M., Wiepjes, C. M., de Blok, C. J. M., Gooren, L. J. G., Kreukels, B. P. C., & den Heijer, M. (2019). Occurrence of acute cardiovascular events in transgender individuals receiving hormone therapy. Circulation, 139(11), 1461–1462. https://doi.org/10.1161/CIRCULATIONAHA.118.038584
Olson-Kennedy, J., Durazo-Arvizu, R., Wang, L., Wong, C. F., Chen, D., Ehrensaft, D., Hidalgo, M. A., Chan, Y. M., Garofalo, R., Radix, A. E., & Rosenthal, S. M. (2025). Mental and emotional health of youth after 24 months of gender-affirming medical care initiated with pubertal suppression [Preprint]. medRxiv. https://doi.org/10.1101/2025.05.14.25327614
Piper, A., & Merskey, H. (2004). The persistence of folly: A critical examination of dissociative identity disorder. Part I. The excesses of an improbable concept. Canadian Journal of Psychiatry, 49(9), 592–600. https://doi.org/10.1177/070674370404900904
Rahman, T., & Abugel, J. (2024). Extreme overvalued beliefs: Clinical and forensic psychiatric dimensions. Oxford University Press. https://doi.org/10.1093/9780197612583.001.0001
Rahman, T., Hartz, S. M., Xiong, W., Meloy, J. R., Janofsky, J., Harry, B., & Resnick, P. J. (2020). Extreme overvalued beliefs. Journal of the American Academy of Psychiatry and the Law, 48(3), 319–326. https://jaapl.org/content/48/3/319
Rahman, T., Meloy, J. R., & Bauer, R. (2019). Extreme overvalued belief and the legacy of Carl Wernicke. Journal of the American Academy of Psychiatry and the Law, 47(2), 180–187. https://jaapl.org/content/47/2/180
Raz, M. (2013). The lobotomy letters: The making of American psychosurgery. University of Rochester Press. https://books.google.com/books/about/The_Lobotomy_Letters.html?id=DG6iAWBlbJgC
Roberts, C. M., Klein, D. A., Adirim, T. A., Schvey, N. A., & Hisle-Gorman, E. (2022). Continuation of gender-affirming hormones among transgender adolescents and adults. The Journal of Clinical Endocrinology & Metabolism, 107(9), e3937–e3943. https://doi.org/10.1210/clinem/dgac251
Rocca, W. A., Grossardt, B. R., de Andrade, M., Malkasian, G. D., & Melton, L. J., 3rd (2006). Survival patterns after oophorectomy in premenopausal women: A population-based cohort study. The Lancet. Oncology, 7(10), 821–828. https://doi.org/10.1016/S1470-2045(06)70869-5
Shumer, D. E., Reisner, S. L., Edwards-Leeper, L., & Tishelman, A. (2016). Evaluation of Asperger syndrome in youth presenting to a gender dysphoria clinic. LGBT Health, 3(5), 387–390. https://doi.org/10.1089/lgbt.2015.0070
Van de Cauter, J., Defreyne, J., T’Sjoen, G., & Aujoulat, I. (2024). Exploring work absences and return to work during social transition and following gender-affirming care, a mixed-methods approach: “Bridging support actors through literacy.” Journal of Occupational Rehabilitation, 34(2), 425–446. https://doi.org/10.1007/s10926-023-10139-x
Van de Cauter, J., Van Schoorisse, H., Van de Velde, D., Motmans, J., & Braeckman, L. (2021). Return to work of transgender people: A systematic review through the blender of occupational health. PLOS ONE, 16(11), e0259206. https://doi.org/10.1371/journal.pone.0259206
van der Schouw, Y. T., van der Graaf, Y., Steyerberg, E. W., Eijkemans, J. C., & Banga, J. D. (1996). Age at menopause as a risk factor for cardiovascular mortality. Lancet (London, England), 347(9003), 714–718. https://doi.org/10.1016/s0140-6736(96)90075-6
Wang, A. M. Q., Tsang, V., Mankowski, P., Demsey, D., Kavanagh, A., & Genoway, K. (2022). Outcomes following gender-affirming phalloplasty: A systematic review and meta-analysis. Sexual Medicine Reviews, 10(4), 499-512. https://doi.org/10.1016/j.sxmr.2022.03.002
Warrier, V., Greenberg, D. M., Weir, E., Buckingham, C., Smith, P., Lai, M. C., Allison, C., & Baron-Cohen, S. (2020). Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals. Nature Communications, 11, 3959. https://doi.org/10.1038/s41467-020-17794-1
Wernicke, C. (1892). Ueber fixe Ideen [On fixed ideas]. Deutsche Medicinische Wochenschrift, 18(25), 581–582. https://doi.org/10.1055/s-0029-1199224
Wiepjes, C. M., den Heijer, M., Bremmer, M. A., Nota, N. M., de Blok, C. J. M., Coumou, B. J. G., & Steensma, T. D. (2020). Trends in suicide death risk in transgender people: Results from the Amsterdam Cohort of Gender Dysphoria study (1972–2017). Acta Psychiatrica Scandinavica, 141(6), 486–491. https://doi.org/10.1111/acps.13164
World Health Organization. (2018). International classification of diseases for mortality and morbidity statistics (11th ed.). https://www.who.int/standards/classifications/frequently-asked-questions/gender-incongruence-and-transgender-health-in-the-icd
World Professional Association for Transgender Health. (2010, May 26). De-psychopathologisation statement. https://wpath.org/wp-content/uploads/2024/11/de-psychopathologisation-5-26-10-on-letterhead.pdf
World Professional Association for Transgender Health. (2016, December 21). Position statement on medical necessity of treatment, sex reassignment, and insurance coverage in the U.S.A. https://wpath.org/wp-content/uploads/2024/11/WPATH-Position-on-Medical-Necessity-12-21-2016.pdf