Brother David: An Ethical Tale, Part 2
By Frank Steiner and Polly Davis

Part 1 in this series presents the case study of Brother David, a monk who asked a urologist to castrate him. After questioning the patient’s sanity, the urologist referred the man for a psychiatric evaluation. Although the patient was found to have no psychiatric illness, the psychiatrist could not recommend castration because of the uncertain effectiveness of the procedure and its unknown long-term medical and psychological effects. Ultimately, an ethics committee concluded that castration was neither medically necessary nor appropriate for Brother David.
Severing Other Healthy Body Parts for Other Reasons
Medical school graduates, including Brother David’s doctors, promise to follow an ethical code. This code obliges doctors to provide respectful care that benefits the patient and avoids harm. Although the ancient Hippocratic Oath comes to mind when considering medical ethics, today’s biomedical ethical standards have evolved over time to include four broadly accepted principles: beneficence, nonmaleficence, justice, and patient autonomy. (Note: Although the ethics committee in Brother David’s case study used a slightly different set of principles, the underlying issues they considered were substantially the same.)
The principle of beneficence obliges doctors to take positive action for their patients’ benefit, promoting good health and removing conditions that cause harm. The duty of nonmaleficence requires doctors to refrain from actions that would cause harm to the patient, including interventions that would kill, cause pain or suffering, incapacitate, or otherwise undermine the patient’s well-being. In addition, doctors must administer healthcare in accordance with justice. This principle exists to ensure that patients are treated equitably and without unfair discrimination. Justice in medical ethics requires that resources be distributed by taking into consideration urgency, scarcity, and severity, as well as individual rights and collective needs, with particular regard to vulnerable patients or those in marginalized groups. Finally, when making ethical medical decisions, doctors must respect patient autonomy. This principle allows patients with the capacity to make their own healthcare decisions to exercise self-determination regarding their medical care. In so doing, doctors must give patients full disclosure of information about their condition, as well as the risks and benefits of available treatment options. In return patients must give informed consent without coercive influences prior to receiving treatment.
These principles are the four pillars of modern biomedical ethics. Together, they constitute a framework for making ethical decisions. However, applying them reveals how they can conflict with one another. A doctor may want to exercise beneficence by administering mechanical ventilation, but the patient may exercise autonomy by refusing the treatment. Amputating a limb could appear to be maleficence because it would result in a disability for the patient, but removing a gangrenous leg may be necessary to save the patient’s life. A patient may exercise autonomy by opting for a new kidney, but the exercise of justice may deprioritize him on the waiting list because he is unlikely to benefit from the transplant. When making an ethical choice, no individual principle should be ignored or assigned undue importance. A physician must weigh each principle and strive to create a positive balance of benefits over risks and costs, while incorporating respect for patient autonomy and justice.
If a patient asks a doctor to cut off healthy body parts, this ought to raise serious ethical questions, as it did in Brother David’s case. Consider patients with Body Integrity Dysphoria (BID), also known as Body Integrity Identity Disorder (BIID), Xenomelia (Greek for “foreign limb”), Apotemnophilia (a sexual fetish), and Amputee Identity Disorder. This condition is a very rare mental disorder characterized by the intense and persistent desire to be physically disabled, usually by the amputation of a limb. Some individuals with BID pretend to be disabled, and some even attempt self-amputation. Individuals with BID are not psychotic or delusional. They are sane and are aware that seeking amputation is not normal.
The cause of BID is unclear. Some research points to evidence that BID has a neurological basis. Other studies indicate that BID is a psychological condition, and have shown that some patients have been able to relieve or end their desire for amputation without medical intervention. Although there is no specific cure for BID, treatments include Cognitive Behavioral Therapy to change distorted thoughts and negative behaviors, and pharmaceuticals for managing anxiety and depression. These treatments have not been consistently effective in eliminating the mental pressure that drives patients to seek amputation. Doctors have occasionally resorted to surgically removing a limb when the patient experiences severe distress concerning an unwanted body part and after other treatments have failed.
Surgical treatment for BID is controversial. Some researchers have concluded that amputation is the appropriate treatment for this disorder, by heavily weighting patient autonomy and the right to modify one’s own body. Other researchers denounce amputation by emphasizing the principle of nonmaleficence, and have pointed out the enormous risks and consequences, as well as the irreversible damage, posed by cutting off a healthy body part. Some argue that amputation is justified and beneficence applies when the patient is so obsessed with their offending limb that surgery is a better option than the risk of self-amputation, for example, by placing it in front of a moving train. The principle of justice, however, cannot support amputation given the high costs of adverse consequences, rehabilitation, lost income, and life-long follow-up.
Several studies have examined the quality of life of patients with BID who have undergone amputation. While some patients reported satisfaction with the amputation, other amputees admitted to personal, social, and financial disadvantages resulting from having a body part removed. Some amputees even expressed the desire for additional amputations! Although surgery can sometimes be an effective way to reduce or eliminate the desire for amputation, it is not recognized by any medical organizations as a standard treatment for BID. Ethical principles as well as potential legal issues such as medical malpractice and assault are obvious concerns that ought to influence the decision of whether to surgically intervene in cases where patients experience BID.
The Surgical Cure For The Mind
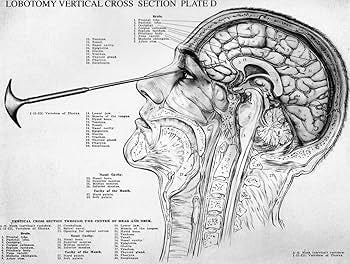
The use of surgery to treat patients with mental disorders has a long history of ethical problems. For example, from the 1940s to the 1960s, lobotomy was a common surgical treatment for severe mental illnesses, such as schizophrenia, major depression, and bipolar disorder. A transorbital lobotomy was performed by inserting an instrument that resembled an ice pick into the brain through the eye socket and sweeping it from side to side to sever connections in the frontal lobe. Although the intervention often made patients more docile and easier to manage, it frequently had debilitating side effects, such as apathy, personality changes, cognitive impairment, and seizures. Lobotomies sometimes turned patients into zombies with vacant stares. Some lobotomized patients lost their ability to function independently and needed to be institutionalized. The outcome could be horrific. Many patients died as a result of the treatment. Lobotomies ultimately fell out of favor by the 1970s and were banned in some countries due to their varied results and severe, long-term, harmful effects. The development of less invasive treatments, including psychotropic medications and therapy, offered safer and more effective alternatives.
Today, lobotomies are recognized as an ethical failure. Observe the practice of lobotomy through the lens of the four ethical principles: beneficence, nonmaleficence, patient autonomy, and justice. Lobotomies were performed without any controlled studies to demonstrate their long-term efficacy and impact. The procedure caused serious harm and resulted in permanent suffering that undermined patient well-being. While doctors may have believed they were taking positive action to benefit the patient, they were careless with regard to patient respect and dignity. Patients were not fully informed about the risks of irreversible harm and were not required to give informed consent. Moreover, the operation was performed on vulnerable, marginalized individuals who were the unfortunate victims of a ghoulish medical experiment.
The four principles of medical ethics had not yet been formalized when lobotomies were performed. However, the failure of this surgical procedure was instrumental in their development. These ethical principles are now used to bring clarity to complex medical problems, such as whether to castrate a healthy man seeking spiritual purity, or to amputate a healthy limb from a person who wants to be disabled. Today, lobotomy no longer poses an ethical question. It has been asked and answered. The ethical analysis of lobotomy provides an important example of how medical professionals’ intention to ease suffering can sometimes cause more harm than good.
To learn more about the authors, Frank Steiner and Polly Davis, please visit their Substack @prankandfolly
Genspect publishes a variety of authors with different perspectives. Any opinions expressed in this article are the author’s and do not necessarily reflect Genspect’s official position. For more on Genspect, visit our FAQs.