The Transition Trap – defining the emotions behind medicalisation
By Vincent Deboni

I have cultivated relationships with many detransitioners in the last three years, including Laura Becker, who spoke to me about topics related to her trans journey and challenges faced by Gen Z on TransPsychePod. At Genspect’s conference in Killarney, Ireland earlier this year, I heard from detransitioners about how they were still lingering in online spaces that were not healthy or supportive. Considering this, Genspect had organised several Google Hangouts meetings for detransitioners in previous months. During late-night conversations over pints of Guinness, we decided to reboot the idea of having a supportive online space for detransitioners. We began meeting regularly in June 2023.
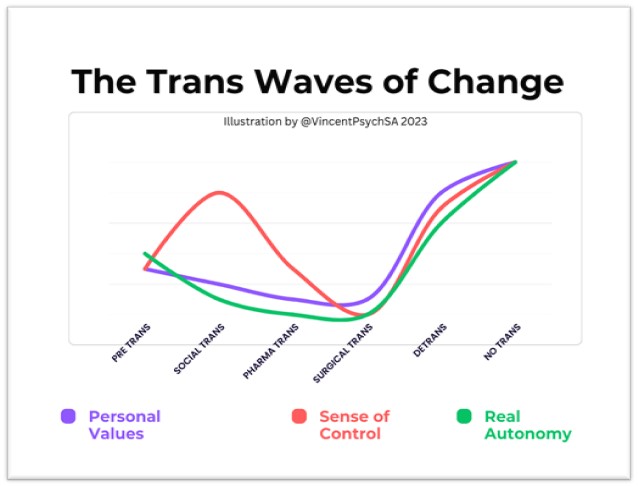
What follows is feedback from the discussions held with the group. A member of the group called Chris, who graciously agreed to be quoted here, summarised the feedback. We discussed the idea of The Trans Waves of Change, presented in the graph below. This is not research, survey results or any data yet, the idea is a work in progress.
In this dialogue, I began by asking the group members what message they would like to send to those who are considering transition.
Chris: I want to talk about how trans identification is an attempt to take control, to take agency, to self-empower. It’s an attempt to control your environment, yourself, and your life. Most people who identify as trans have experienced a feeling of powerlessness, a feeling of lack of control, and of lack of agency. They’ve felt like they were marginalised; this probably started young in life. When they identify as trans, they’re following a program, a step-by-step program of taking action, doing things that they can use to try to bring them a sense of control and safety through that control. So, when they start following these steps each step can feel empowering and it likely is empowering. They’re doing things that make them feel like they’re expressing themselves, like they’re asserting themselves in the world, in their environment, and against other people’s pushback. That’s empowering.
Me: So, this doesn’t sound so bad, getting more control of your life could be enabling. In my work I often come across people who have no autonomy, it is very unhealthy, maybe social transitioning is harmless?
Chris: The problem is that one of the stages in this process is medicalisation. Up to medicalisation, they feel empowered when they do social things, like changing clothing, changing pronouns, telling people that they are one gender or the other. Whatever it is, they fully control that process. They believe they can stop any time they want. They can change it any time they want. They could go as slow or as fast as they want. They are in control. That’s why they feel in control. It’s self-expression.
Me: You make it sound like it is a trap?
Chris: The medicalisation stage is the trap, it creeps up on them because of that initial boost in self-confidence, they feel invincible. They follow the steps, change their pronouns, change their gender and how they dress. And then they ask, “What’s next?” The medical pathway provides them with the next stage, which is cross-sex hormones. This stage appears to be the ultimate expression of self-control because it takes control of the body directly. Within transgender communities, it is represented as self-affirmation through subjecting your body to your own will, and it is backed by the appearance of medical certainty.
Me: It sounds like a well-designed incentive and reward system, promising a kind of ‘life after death.’ I experienced this when I was anorexic in my early adulthood. I believed if only I could eat the purest, healthiest, most harmless foods I would be worthy of love. How does this differ from the futile pursuit of an anorexic? Why is it so dangerous?
Chris: It is dangerous because they believe going into it that they are taking control of their biology, but they are wrong. They believe they will make their bodies do what they want them to do, but they don’t understand that your biology and the transition drugs do things that are completely independent of your will. If you take them for the wrong reasons, it means that you will not get what you’re expecting or what you want out of them. As soon as you take those hormones, your body starts doing things that are completely beyond your power. You effectively lose power: you lose control, you lose agency. You have all that dysphoria flood back into your life. That’s why so many people start taking hormones and within six months they say things like: “I can’t do this anymore. I feel horrible. My dysphoria is back. I hate this.”
Me: It sounds like an obsession that has taken control of someone’s life. We spoke previously about obsessive-compulsive disorder (OCD) in those who attempt to transition, why do you think it is so common?
Chris: Because OCD or obsessiveness is an attempt to control, to take control of your environment, to control things through rituals. It’s an attempt to follow these rituals that are going to make you feel safer, and this is part of that. They’re obsessing over something to the point that they take medication to relieve the anxiety. This is putting the drug in the driver’s seat.
Me: We see many people who develop unhealthy habits to soothe existential angst, you have people who self-medicate with alcohol, weed, and benzodiazepines or use devices to deflect from their discomfort. In this case, why is it a bad strategy?
Chris: It goes back to the concept that this stage of transition is a trap. You go into it thinking you’re going to gain control of yourself, but it’s going to do things to you that you can’t stop when you want to, which you can’t change when you want to, which go at a pace that you can’t control. It will likely be very, very fast. If you’ve been enjoying a slow, gradual build-up in your life, suddenly this thing is going to hit you hard in a way that you can’t do anything about. When it hits you, you just go along with what it does to you. You must experience what it does to you, and you must feel the way that the world and other people react to what it does to you. You will have no ability to change that or to wrest control back from it.
Me: Then this phase effectively strips you of your identity? I often talk about how we must remain in control of the source of our dopamine. If we hand over control of our dopamine, we surrender our motivation to an external force. This sounds like a whole new way of robbing someone of their motivation.
Chris: In a way, the person is subjecting their identity to the treatment. They’re hoping this will make them feel more agency like social transition might have, but this is not something that is at all like their prior experiences with social transition. Medicalisation takes the agency out of your hands and puts it in the hands of the drug that you are taking. It hijacks you physically. Your philosophy and your theories are all subject to the process. They don’t matter. Your feelings don’t matter. The drug doesn’t care how your body reacts to it, it doesn’t care if you suddenly feel dysphoric, if you feel worse than you did before. It will keep doing what it’s doing. If you stop taking it, you won’t just go back to normal. You won’t immediately lose the effects. These drugs last in your system. If you were taking something like Nebido (synthetic testosterone), which lasts up to three months in your system, you’re going to be affected by that for the next year. And if you stop with these drugs, you will have permanent effects that will take years to start to show even a little reversion. And even then, you may never fully recover. People need to understand why people are motivated to do this in the first place; and why they think it’s safe and reasonable to try out. And they need to understand that nothing can prepare you for this negative outcome.
Me: Let’s talk about the graph here, what are your thoughts?
Chris: I would say that the implication that personal values and real autonomy drop during social transition is a reasonable assertion, given what I know about your psychological beliefs about these concepts. The idea that one’s sense of control increases is completely correct. The idea that one reaches a peak in this and then moves toward pharmacological transition is interesting. Your graph suggests a constant decline in sense of control, but what we’ve often found is that people recurrently affirm their sense of control through their transition efforts. They do things like pharmacological self-modification to regain the sense of control they had at their peak. Indeed, they probably do regain some control, since it is entirely subjective and vulnerable to placebo.
Me: What about the personal values track?
Chris: The idea that during this stage a person’s values are degraded and their autonomy drops suggests to me that you believe that a person is continually subjecting their values to the values being imposed on them by the transition process. This is interesting. The most common path indeed is for people to be drawn deeper into the ideological convictions that surround transition, so this may be true. The transition stage itself may not cause this but rather transition is caused by a stronger commitment to the belief system. The belief system uses transition as a ritual affirmation of beliefs, which in turn is why the sense of control increases. One feels temporarily accomplished at each stage.
Me: Yes, I have deliberately shown a drop in values because my work with detrans and trans people revealed this. It is common in many people, but in this case, they are adopting the values of an ideology, which will lull them into a false sense of security. Only when their values are revived can they begin to exercise meaningful control again, which will lead to genuine autonomy.
Chris: Regarding autonomy, it is objectively correct that someone who subjects their values to a group belief system loses autonomy. It is interesting that this line is separate from value degradation. My best defence of this is that personal values are not entirely lost when one becomes part of a group belief system, but they do become further apart from one’s own best interest. Perhaps we could say that a person’s actual autonomy is relatively more dramatically impacted by their beliefs being subverted in this way.
Me: I believe value-less autonomy is merely chaotic freedom. Autonomy requires agency or power to act on your choices. A person who acts irrationally or unpredictably—as one would if they had no values—is going to lose power because they will be ostracised and isolated by the natural order of human responses to these existential threats. It is human nature to avoid someone who appears to make choices without prosocial values.
Chris: Your graph suggests that all values, most notably sense of control, bottom out at the point of surgery. I believe the sense of control peaks for many transitioners when they have surgery. I think that by the time they get to surgery, they have already experienced a complete loss of sense of self-preservation, personal values (vs. the values of the belief system), and true autonomy. They have, essentially, placed themselves entirely at the whims of medical professionals. They have probably resigned themselves to a kind of blind faith. I must say, however, that not having reached this point myself I am not qualified to speak accurately on the state of mind of someone who has. This conjecture on my part is a projection based on my path and extrapolation of the stories I have heard along with personal philosophy.
Me: Speaking of faith, Professor Lisa Miller writes about how we develop faith in our choices by exercising our spirituality. She talks about intuition and serendipity. Her research revealed differences in the brain between people who use both modes to make choices: objective and intuitive. So, we could say faith has been misplaced in the trans pipeline. Surgery becomes the final ‘Hail Mary’ to reach heaven.
Chris: The graph seems to suggest that when getting surgery their lives become much better. It is likely that post-surgery there is an increase in sense of control but it will decline over time. The other values probably stay low. The reason for this is that we don’t just get mentally better as we approach detransition, in my opinion. We reach a point where we have become unable to ignore the degradation of our autonomy and personal goods, among other things, which leads us to the realisation that we have been wrong, and that we must try to fix our circumstances. This is important to note because the final stage you have is “no trans”, which I think implies that we detransition into a state of no longer being trans. I see trans as meaning transgender, and I see transition as separate from transgender identity. That being the case, a person might detransition, change many of their beliefs, and still acknowledge some kind of gender identity or nonconformity or some sort of trans-adjacent theory. I do not think all detrans people will even give up trans identities. I think the trap of transition is that it takes advantage of identity beliefs to trick one into medical procedures, which are an entirely different ball game.
Me: Yes, I see what you are saying, each person has their journey, the graph is just to illustrate common pathways. I suppose detrans is not an identity, otherwise we would be repeating the same errors made during the trans phase?
Chris: It may be the case that some will no longer identify as trans after detransition, but I would suspect that for those who give up the identity it is very quick and might even precede detransition. The beliefs need to change before the practices do, or at least in tandem with lifestyle changes. The change in views motivates the change in medical decisions. It is also necessary to note that a person does not ever stop being detrans once they have become detrans. You are always detrans because it is a description of the medical state of your body.
Me: I like that, it describes an experience you had, not the person you are.
Chris: Exactly! Similarly, an amputee will be an amputee regardless of other changes in their life and regardless of their mental attitude about it. They may not identify with such a description, but it does objectively describe their body. This is again where the earlier distinction is important because a detrans person is detransitioned, not de-transgender, which is not a thing to my knowledge.
Me: I think detransition can be a phase in the sense that the person is undergoing a true metamorphosis into adulthood, into self-actualisation. Many detrans people need support during this phase.
Chris: Some will still end up with many of the same problems they had before they transitioned and detransitioned, but they will be closer to addressing those problems now that they are not using snake oil as a treatment. They have more opportunities to choose a successful path.
Other participants added their feedback, some said that the first wave represented by the spike in Sense of Control reveals the first lie that trans ideology is pushing. One said her values returned as soon as she accepted it was all a “scam”, another noted that the rise in a Sense of Control depends on how your community responds, some people will gain more of a sense of control in very accepting environments. Of course, this should not be misinterpreted; affirming environments will increase the power of the lie. This tells us that we must stop allowing the lie to be told. Once we collapse the first wave, we invite the second wave, where personal values, real control and authentic autonomy can blossom.
Interview with Chris @DefinedUniquely Written by Vincent Deboni
Photo by Lance Asper on Unsplash