Don’t Try to Stop Me or I’ll Kill Myself
By Anonymous

A few years ago, when I knew much less about all this than I do now, I had my first meeting with a gender therapist.
Our teen daughter had hit a rough spot. Struggling socially and academically in a new school, she learned a novel idea from her peers: she could be transgender. While at first blush it rightly struck her as crazy, after some months of quiet rumination together with the internet and the coaching of new friends in the school GSA club, she started to see that theory as an explanation for much of her unhappiness. She “came out as a guy” to friends and a sympathetic teacher at school, and then to us, her parents. We saw this announcement within her larger developmental context as a confused reaction to not-so-exceptional teen angst and some recent unwelcome sexual attention. One thing that’s been clear about our daughter from infancy is that she can be very stubborn and resistant to following direct advice. That’s not an uncommon fault in bright and independent children. We had confidence that given some time and maturity she would figure out on her own that the idea that she is really a man is nuts. However, under the zeitgeist of the time and on the advice of “professionals” we acceded to our daughter’s request to see a gender therapist on the assumption that this person might actually help her sort things out.
At the initial meeting the gender therapist sized us up as doubtful and talked a good game: she claimed to be very careful and open minded and wouldn’t jump to conclusions; she wanted to extensively explore all the relevant issues. Still, it struck me as odd that she already seemed to be testing our receptivity to the idea of going along with hormones and surgery. Towards the end of the meeting she hit us with the hammer. Maybe we had not shown sufficient faith in the wisdom of the affirmative approach. She leaned over, pinched her face into an expression of deep concern, lowered her voice and dramatically uttered, “One thing we do know is that these kids attempt suicide at incredibly high rates.” The implied message was as clear as it was shocking: Listen to us experts. If you don’t accept your daughter as a boy and allow her to proceed with medical interventions, there’s a good chance she will kill herself.
Every parent with a gender-confused child has heard some version of this threat from multiple sources. It’s part of what Everybody Knows because Experts Say So. It’s also a big part of how the radical Affirmation Only approach has steamrolled over all resistance to become the de facto policy of nearly every relevant major institution in North America.
The basic argument for Affirmation Only is roughly this:
- Untreated gender dysphoria leads to an extreme suicide risk.
- Medical transition (in conjunction with social acceptance) is the only effective treatment for gender dysphoria.
- Therefore: The benefits of offering medical transition on demand outweigh the expected likelihood of medical risks (like damaged health or regret).
Both premises of this argument are false but the first one has been particularly effective in persuading people who should know better to look the other way, to forgo due diligence, and to accept surprising new policies on only the skimpiest evidence. Questioning the actual evidence that is supposed to justify Affirmation Only policies is rarely met by good faith discussion of the nature and strength of that evidence. Instead the person raising such questions is much more likely to be accused of being motivated by bigotry and of perpetuating immoral beliefs directly responsible for many suicides (and even murders), deaths that would not occur if society would only universally affirm gender identity and offer medical transition on demand.
This is the suicide myth I want to examine. The vague but ubiquitous presumption that the risk of suicide by trans-identified people, especially youth, is so extreme that it justifies bypassing established standards of decision making whenever those standards pose a barrier to immediately gratifying the trans-person’s desire for medical intervention or social accommodation.
The suicide myth is an adult version of how a child blackmails his parents with a tantrum, and it too often works. Look around: How many people are willing to risk the career damage of being tarred as a transphobic bigot in order to challenge the recommendations of some special interest committee when ignoring it or nodding along can be rationalized as probably not having much real consequence anyway?
The rest of this essay is going to look at how the suicide myth has come to be so widely believed and why the medical professionals using it to argue for Affirmation Only must be considered either derelict in their professional competence or, worse, deliberate charlatans.
A Brief History
The association of suicide with transsexual behavior goes back at least to the mid twentieth century when previously taboo sexual subjects began to attract more academic attention. In the 1940’s Alfred Kinsey began publishing research into sexual practices, including some that had long been considered deviant. In that period general advances in drug synthesis and surgical techniques made it possible for the first time to medically alter some of the visible sex characteristics of the human body. A few doctors began offering cross-sex hormones and cosmetic surgery to patients who expressed a strong desire to become the other sex. One of the early proponents of such treatment was Harry Benjamin. In 1966 Benjamin published a book titled The Transsexual Phenomenon that laid out his theories, based on reportedly having seen roughly 200 patients expressing a desire to change sex, of whom about 70 underwent surgery toward that end. Describing the psychological profile of these people he wrote:
There is hardly a person so constantly unhappy (before sex change) as the transsexual….the transsexual’s gender disharmony…makes him forever a candidate for self-mutililation, suicide, or its attempt. The false relief obtained from alcohol and drugs is not an infrequent complication. (p30) To their families these transsexuals are often an enormous problem. …[They may] threaten suicide when opposed too much. (p31)
Benjamin was very sympathetic to the transsexuals he studied and advocated for more widespread provision of medical transition services. He believed the acute unhappiness of pre-operative transsexuals was fundamentally due to the incongruence between an inalterable inner sense of self and the physical body, and that suicidal tendencies should be attributed first to that cause. He argued that medical transition was more effective in relieving that unhappiness than any known psychotherapeutic techniques of the time. He did note that a significant minority of the patients he observed continued to exhibit mentally disturbed behavior after transition. He also recognized that the evidence for his recommendation was largely anecdotal and based on short-duration observation, and that future research might draw a different conclusion:
It is not too difficult to visualize a possible future when extended scientific investigation might show that transsexual patients in the end – say after twenty years’ observation – had not been materially benefited by the surgical alteration of their genitals. In such case, the operation would fall into disrepute and would be largely abandoned. (p67)
Prior to 1960, Americans desiring a “sex change operation” needed to travel to Europe or North Africa, since such services were not openly available in the US. Common opinion in the medical establishment did not view it as a legitimate treatment. However, opinion liberalized during the 60s and 70s and multiple US clinics began to offer hormonal and surgical therapies for what came to be known as “gender dysphoria.” This included highly reputable institutions like Johns Hopkins, where the controversial John Money founded his Gender Identity Clinic in Johns Hobkins, Baltimore and it was officially established in 1966. This was the early “gatekeeping era” of what later came to be known as transgender medicine.
The early clinics wanted their foray into this new field to be judged ethically and medically responsible, so they attempted to vet applicants and admit to treatment only those for whom the chances of a positive outcome appeared most likely. Since there wasn’t any solid research to guide these decisions, doctors took their best guess at sensible criteria. For example, concerning physical characteristics, men desiring to transition to female were less likely to be accepted if they were very tall or overtly rugged looking, since the likelihood of successfully “passing” after surgery seemed lower. As for psychological criteria, Benjamin’s theories became influential. Clinics found that many applicants fit the profile described in his book: claimed opposite sex identification since early childhood, despondent to the point of suicidal ideation, but otherwise seemingly fairly normal. Eventually clinicians learned that Benjamin’s book had been widely read by those aspiring to treatment and that this community coached one another on how best to approach the clinics. A 1972 New York Times article reported:
In retrospect, the centers are pleased with their conservatism, for they see now how easy it is to misdiagnose transsexualism and consequently perform irrevocable surgery on the wrong persons. “We have to be especially careful now,” said Dr. Jon Meyer, who heads the Johns Hopkins program, “because the word is out on how to talk to the doctors to perform the surgery.”
So right from the start of medical treatment for gender dysphoria there was a perception of elevated suicidality among the patient population, yet there were no good studies providing answers to any of these pertinent questions: What motivates self reports of suicidality by applicants to gender clinics? To what extent are they truly organic expressions of a patient’s mental state versus an attempt to fulfill expectations or to bargain with gatekeepers? To the extent factual, what are the causes of these behaviors, what is the mixture of unhappiness with one’s own physical characteristics versus lack of social acceptance versus other possible psychological problems or mental disorders? Does the idea of transsexuality attract people who are mentally disordered and already prone to suicidality for other reasons? To what degree does the expression of suicidality predict actual completed suicide in this population, versus in the population at large? Regarding the actual likelihood of serious self harm, to what extent is it reduced in the long run by medical transition?
In the mid to late 1970s there was a wave of closures of gender clinics. 1 Most famously the clinic at Johns Hopkins was closed in 1979 following the publication of a paper by Meyer and Reter titled Sex Reassignment: Follow-Up which reported that medium term (2 to 5 year) follow-up of patients failed to show that gains in well-being could reliably be attributed to receiving transsexual surgery. Their study incorporated two features not seen in more recent studies purporting to demonstrate such gains. First, they attempted to measure objective criteria correlated with well-being, like stable relationships and employment, rather than subjective reports of being satisfied with the outcome of treatment. Secondly they included a large comparison group (2x) of people who had sought transsexual surgery but not received it. Their major finding was not that the surgery group didn’t improve, but that the no-surgery group also improved in well-being at follow-up, to a level not significantly different from the surgery group. In other words, there was no evidence that surgery improved outcomes any more than just time and some professional attention. 2 Weaknesses of this study include small sample size and high loss-to-followup, weaknesses common to almost all outcome studies in this field. However, critics also accused the authors of bias, arguing that this study and many of the clinic closings were motivated more by ideology (in this case religious conservatism) than actual evidence. In 1978 the Harry Benjamin International Gender Dysphoria Association (HBIGDA) was formed to foster communication among those continuing to practice in the field.
The period 1980 to 2000 saw a slow expansion of gender medicine availability under continued gatekeeping by medical professionals. The same period also saw growth in organized activism aimed towards social acceptance of homosexuality and better medical care for AIDS. A similar activism, eventually framed in terms of civil rights, began to arise among transsexuals and their sympathizers. The early activists were mainly natal males who sought transition to female as adults. Their desires included eliminating gatekeeping for medical transition, having the costs covered by health insurance, and gaining legal and social recognition as legitimate women. Many also argued that their gender identities were innate and stable since childhood, and their lives would have been better had they been able to transition earlier, as minors. Thus they argued for medical transition for minors. HBIGDA was a natural focal point for these new “trans activists” as they came to be called, and the successful gay and lesbian rights movements were seen as models and potential allies to which they might attach their own movement.
Over a few years around the year 2000, HBIGDA underwent a distinct change in orientation. The organization had originally been founded to improve medical practice in its subject area. Its early membership was predominantly practicing clinicians. Trans activists began attending meetings and demanding that their personal testimony should be given more weight than traditional types of medical evidence. As those with a more activist outlook gained influence, the agenda, name and overall membership of the organization changed significantly. Voting membership was opened to people holding a much wider and less selective range of credentials (e.g. social worker), relatively few of whom had pertinent clinical experience or demonstrable ability to evaluate the merits of complex scientific arguments. The agenda shifted to one originating with trans activists, rather than clinicians or researchers: normalizing transgender identification and behavior, and making medical transition affordable and easily obtainable. Reflecting this change, a new name was adopted: the World Professional Association for Transgender Health (WPATH). Some existing members of HBIGDA who disagreed with these changes either resigned or were forced out. (The evolution from HBIGDA to WPATH is touched on in a legal deposition of Stephen Levine, and in the book Galileo’s Middle Finger by Alice Dreger.)
Today’s WPATH is properly viewed not as a dispassionate, science-led medical organization, for which it would like to be mistaken, but rather as an activist organization with a particular agenda for changing medical care that is not supported by adequate evidence. Towards that end it fosters the production of scientific appearing publications that agree with its goals (e.g. through publication in affiliated journals like the International Journal of Transgender Health and Transgender Health). It also attempts to influence the policies of medical societies by framing its own positions as evidence-based and authoritative, and having its members seek positions on committees that craft policies related to gender medicine. 3 In addition to adopting the agenda of transactivists, the Affirmation Only movement championed by WPATH has adopted some of their long-time tactics, particularly the use of suicide threat to manipulate other parties into abandoning normal due diligence and acceding to their demands. Exaggerating the risk of suicide in trans identified people has been used to argue for on-demand “informed consent” provision of experimental and irreversible medical treatments, for social and medical transition of minors without parental consent, and as a tactic to suppress open and balanced discussion of these issues. Exaggerated suicide risk is the main tactic used to argue for experimental interventions with little proven benefit and likely risks, and against withholding those interventions from a control group, making it impossible to carry out controlled studies similar to Meyer and Reter 1979 that might demonstrate those interventions to be useless or worse.
Motte, Bailey or Straw Man?
Let’s test your snap intuition. An advocacy group for disabled veterans of a recent unpopular war announces “Studies of this extremely vulnerable group show that a shocking 40% have already attempted suicide.” Based just on that information, make an initial guess as to the percentage of the group that will eventually die by suicide. Is it 40% or above? Around 4%? Or perhaps no more than 0.4%? In your imagination, how do you picture one of them attempting suicide? Save this thought, we’ll get back to it in a moment.
A common technique in polemical discourse is to deliberately misrepresent the opposing side’s argument in order to construct an exaggerated “straw man” version that is easily demolished. My intention in this essay is to avoid resorting to any such cheap trick. That takes a little work because the myth I’m trying to dispel is communicated largely through suggestion, by framing claims in a way that encourages erroneous assumptions. The actual suicide-relevant claims made on public record by the professional advocates of Gender Affirmation are often a deliberately poor interpretation of evidence, but rarely a bald contradiction of verifiable facts. A useful way to understand what’s going on is to see it as a form of motte and bailey tactic.
The Motte-and-Bailey Fallacy is a style of argument that attempts to establish acceptance of an aggressively broad and indefensible thesis, while falling back to defend only a much narrower thesis when challenged to show evidence. The motte is the cramped and unsatisfying claim that can actually be defended while the bailey is the broader and more radical belief an influencer would like you to accept.
In the context of gender affirmation, the bailey is the expansive belief that extreme suicide risk justifies Affirmation Only policy across all of society, including medicine. It posits that lack of social and medical accommodation causes persons with gender dysphoria to commit suicide at extremely high rates (i.e. these factors independently and significantly increase the real suicide rate). Additionally, it implicitly holds that the aggregate harm of suicide that can be reduced by social and medical accommodation is greater than the aggregate harm (health damage and normal life opportunity lost) that may be increased by on-demand medical transition. In contrast, the motte consists of much more modest claims such as people who self identify as transgender also self report suicidal ideation or unsuccessful attempts at higher than normal rates, and blame it on lack of acceptance. The large gap between the bailey and the motte begs that we address these questions: How predictive of completed suicides are self-reports of suicidal ideation or attempts? How reliably can we attribute suicidality of trans identified people just to lack of social acceptance and medical transition?
The main thrust of the rest of this essay is to argue that the evidence that Affirmation Only will reduce real suicides is extremely weak, and the risk of trans youth suicides has been greatly exaggerated. I also believe it is appropriate to hold the advocates of AO accountable for propagating a dangerous lie based on their deliberately appealing to an exaggerated risk while simultaneously downplaying or denying very real risks of affirming. Towards that end it’s useful to consider what part of the bailey supporters of AO ought to be held accountable to defend, so long as they persist in encouraging the suicide myth.
What was your guess for the question above about disabled veterans? It probably had a lot to do with your familiarity with the subject at hand. Maybe you’re a veteran yourself with relevant personal experience or have previously given similar questions considerable thought. Or maybe you’re not, and you’re inclined to trust experts, and it’s easy for you to imagine a combat veteran with a firearm successfully committing suicide on the first try. In the second case, I’ll bet your guess was at least 4%. What people hear and understand from such a story depends a lot on their context and what they are prepared to believe. It is shaped by what they desire and what they fear.
In 2011 an activist group published a report based on a convenience survey that claimed 41% of all transgender people had attempted suicide at some time in their life. This report was widely trumpeted by sympathetic media and has been very influential in shaping subsequent discourse. It’s impossible to have any skeptical interaction with a gender affirmative therapist or physician without soon being admonished with the extreme suicidality of unaffirmed trans youth, often citing a specific suicide attempt rate around 40%. Therapists and gender clinicians have become accustomed to citing suicide risk as a technique for neutralizing the resistance of parents and colleagues.4 Parents of trans identified children, both those who affirm and those who are skeptical, widely report this experience and the horror they felt on first hearing it. This study and a few similar are the cited evidence basis for the ubiquitous “Better a live son than a dead daughter” argument that has swayed many doubtful but worried parents into affirming transition. The specter of a serious suicide risk also has been used to induce most of the medical profession to look the other way, not to question the conclusions of special-interest committees within medical societies that recommend Afirmation Only policies, and to go along with routinely referring gender questioning youth to doctrine-conforming specialists. Since the suicide myth has become so central to the narrative about transgender youth, adolescents are very aware of it and probably more inclined to express suicidality in order to confirm their true trans nature.5 One of the authors of that 2011 report wrote a subsequent paper6 celebrating the effectiveness of the first report in shaping policy and behavior. Its abstract approvingly describes the grandfather of a trans-identified child becoming emotionally overwrought, desperate for strategies to “keep his granddaughter alive.” That man loved his granddaughter dearly and had been stunned by the revelation of a shocking, hidden danger. What odds of eventual suicide do you suppose he was effectively acting on, if not necessarily consciously accepting?
Although I don’t know of a study that measures the median suicide risk assumed by naive people when first exposed to the 41% claim (fun project for a social scientist?) I’m going to propose a 4% risk of suicide by age 25 as a plausible low-end estimate. It is well established that full cognitive maturity is not generally reached before age 25, and doctors are very reluctant to offer sterilization procedures to anyone under this age. It would seem very reasonable to delay permanent transgender medical interventions until this age, given undeniable evidence that desistance and detransition occur at significant rates, and the lack of proven diagnostic criteria for transgenderism. Yet widespread anecdotal evidence exists that fear of youth suicide in particular has encouraged many parents to consent to medical interventions for their child that pose serious adverse consequences including sterility, loss of sexual function, permanent medical dependency and shortened lifespan. People don’t sterilize their children or damage their endocrine systems in order to reduce their risk of traffic accidents, drug overdoses, or any of the other major risks faced by youth. Many people seem to perceive the trans suicide risk as much, much higher, and advocacy groups encourage that belief. A 2012 publication by a Canadian trans-advocacy group claimed that trans youth “unsupported” by their parents attempted suicide at 15 times the rate of those who were “supported.”7 That comparison was cited by the 2018 position paper on gender medicine by the American Academy of Pediatrics. Quite a few quantitatively naive people seem to accept the completed suicide risk itself as close to 40%. But it’s not necessary to insist on such an extreme value to see that the suicide myth argument is unreasonable.
By the way, what would your snap intuition have been if the advocacy group issuing the report was a high-school psychology club and the vulnerable population studied was adolescent girls who affected goth fashion?
Where Are the Bodies?
Let’s work through a simple rationality check of a kind that anyone who’s passed a rigorous science course at the high school level ought to be able to perform. Given what we actually know about reality, to what extent is it possible that the trans youth suicide narrative could be true?
As an exercise, assume the core claims of the Affirmation Only argument: Transgender identity is innate, unaffected by social influence and unmistakable to the individual upon introspection. Some fraction T of the population has always been transgender. Also, unaffirmed transgender people who do not receive the social acceptance and medical transition necessary to live as their true selves are prone to despair that cannot be ameliorated by purely psychological interventions and commit suicide at an elevated rate of at least S by age 25. What observable consequences should follow?
Prior to 1950 there was almost no recognition of let alone social acceptance for transgenderism in western society. Male and female social roles, conventional dress and expected comportment were strongly differentiated. According to the minority stress hypothesis it should have been a hellish time for the invisible transgender population resulting in a maximal suicide rate. Since the 1960s recognition and acceptance of transgenderism has steadily increased, most dramatically over the past 20 years. Medical interventions have become widely available on demand for those over 18, the media celebrates transgender icons, and nearly all educational and medical institutions are actively seeking to support trans youth. All of this implies that historically measured suicides should upper bound the variables T and S, the size of transgender population and its real propensity to suicide, and if their product is greater than miniscule, suicide trends should reflect the improved prospects created by the gender affirmation movement. The innate and not-socially-influenced nature of transgenderism also implies that any credible survey of self-reported rates of transgenderism should establish a lower bound on T applicable to any other time period as well.
Statistics on death by suicide have been recorded for the United States since at least year 1900. Annual suicide rates are conventionally reported on a per 100,000 population basis. Over the 20th century the suicide rate for the full population varied from a high of 17.4 in 1932 to a low of 9.8 in 1957. The period 1900 to 1940 showed two large peaks in the suicide rate around 1910 and the great depression. These were both periods of great social upheaval.
From 1945 up to the year 2000 overall rates were steadier and much lower than in the first half of the century. Since 2000 there has been an increase in overall and some specific suicide rates. A couple of important observations can be made by considering differences over time and by subpopulation.
Rates can vary significantly by demographic group. Males consistently commit suicide more often than females, recently by a factor of about 3.5. Rates vary across age groups. Rates vary by racial/ethnic group. Non-hispanic whites commit suicide at twice the rate or higher than blacks, hispanics and asians.8 Rural versus urban rates vary, with significantly higher youth suicide rates in rural states than in states with large urban populations.9
Rates increase with age, though youth rates have jumped since about 1950. Prior to mid-century, aggregate suicide rates increased significantly and monotonically by age group. Since then rates for the elderly have declined somewhat, perhaps due to better healthcare and social welfare, while youth rates have increased, particularly for males. For both sexes under age 15 suicides are quite rare. Male rates rise monotone with age and peak above age 75.10 Female rates rise to middle age then descend above age 64.11
Let’s focus on the US male and female youth (age 15-24) suicide rates in the years 195012, 2000 and 2020. Here they are, per 100,000 population.
| 1950 | 2000 | 2020 | |
| Male | 6.5 | 17.1 | 22.4 |
| Female | 2.6 | 3.0 | 5.8 |
There is no visible decrease in youth suicide rates corresponding to greater social and medical accommodation of those identifying as transgender. Not at the granularity of these aggregate statistics. Either some other, unidentified trend towards increase has cancelled out the expected decrease, or else the size of the transgender population multiplied by its actual excessive suicide rate is negligible. One striking fact is that the female youth suicide rate has doubled during the same period when the number of female adolescents identifying as transgender has increased by a large factor, reversing the historical sex ratio of youth claiming an opposite sex identity.
Since 1950 estimates of the size of the transgender population have gradually increased at the same time there has been increased campaigning for greater social acceptance. Starting in the 1960s estimates were made on the basis of visits to health professionals specifically for transsexual care. Estimates by this method varied significantly between countries and publications.13 Early estimates for females (i.e. FtM) ranged from 1 in 400k up to 1 in 100k. Early estimates for males (MtF) ranged from 1 in 100k up to 1 in 35k. By the 1990s one study in the Netherlands estimated frequencies of 1 in 30k for females and 1 in 12k for males.14 Since the year 2000 estimates have often been published by advocacy groups or government agencies on the basis of survey data. The Williams Institute is a prominent source of such publications. In 2011 they estimated that 0.3% (equivalent to 1 in 333) of the US population is transgender.15 In 2016 they estimated 0.6% based on 2014 survey data.16 A 2022 Williams Institute publication reports an increase in those aged 13-17 claiming a transgender identity to 1.4% nationwide with dramatic regional variations from 0.6% in Wyoming to 3% in New York.17 An independent 2022 study by The Pew Research Center reports even higher rates of 1.6% for the whole population and 5% for those in the 18-30 age group.18
If we accept the Affirmation Only premises that transgender identity is innate, not socially influenced and reliably diagnosed through introspection from an early age, then what should we make of these wildly differing estimates? Advocates of AO have consistently refused to acknowledge sharply rising rates of adolescents (especially girls) claiming a transgender identity as evidence of social contagion or anything other than an oppressed minority that has always existed, finally feeling enough acceptance to come forward. Hence it seems fair to evaluate values all the way up to 5% as claims of the true size of the transgender population.
A Simple Mathematical Model
Given the assumptions made by the Affirmation Only model, the historical number of transgender youth committing suicide should average around a value determined by the natural size of the transgender population and its inherent suicide risk, when not ameliorated by social affirmation and medical transition. Presumably some transgender individuals will at times be subject to additional negative influence through circumstances of economic or social hardship, but the basic assumption is that unaffirmed transgenderism is such a potent cause of suicide that it should stand out over time above other causes. The expected annual count of trans youth suicides (per 100k) is given by
Ct = 100000 * T * S/10
where 0 ≤ T ≤1 is the fraction of the population that is naturally transgender and 0≤ S ≤1 is the expected fraction of those persons that will commit suicide in the 10 year period between ages 15 and 24. This must be bounded by the actual observed suicides R (count per 100k) for the age cohort and an estimate of the maximum fraction of those suicides that are primarily due to unaffirmed transgender identity 0≤ Pt ≤ 1.
Ct <= R * Pt
Let’s add a scaling variable I (for infeasibility) to convert this bounding inequality to an equality, where the constraint is satisfied whenever I ≤ 1.
Ct = I * R * Pt
If I > 1 then it indicates the factor by which Ct is infeasibly large, given the other parameter values.
What is a reasonable value for Pt? As mentioned above, the US youth suicide rate has increased significantly since 1950. Consequently there has been considerable academic attention paid to the subject. I randomly selected and read several highly cited studies19,20,21 on this topic published between 1987 and 2001. They contain consideration of a number of plausible causes for youth suicide but transgenderism (nor anything similar like minority sexual orientation) is never mentioned. It seems reasonable to assume that if distress due to transgender identity were the predominant cause of a significant proportion of youth suicides through the 20th century the issue would have attracted notice and appeared in some form in these analyses. There have also been several studies which specifically sought to identify sexual minority youth suicide rates by “psychological autopsies”, all of which found that “same-sex sexual orientation is not disproportionately represented among suicide victims.”22 So it seems safe to assume that Pt <= 0.1. It seems most likely that the true value is much lower than this upper bound, probably even less than 1%.
Solving for a natural transgender rate of 5% and a trans youth suicide rate of 4% yields an expected annual trans-only youth suicide count of 20 per 100k overall population. Calculating with the 1950 male and female suicide rates yields the following infeasibility factors:
Imale = Ct ÷ (R * Pt) = 20 ÷ (6.5 * 0.1) =31
Ifemale = Ct ÷ (R * Pt) = 20 ÷ (2.6 * 0.1) = 77
In both cases the predicted values are much larger than observed values, which makes the assumed T=0.05 and S=0.04 values grossly infeasible. They are nearly as inconsistent with the observed suicide values for years 2000 and 2020, though of course the AO assumptions require the formulas to hold just as well in the past. If we were to entertain estimated trans youth suicide rates of 10% or 40% then the implied trans youth suicide counts would be 40 or 200 which exceed observed values by even larger infeasibility factors of 150 to 700.
When we interpret Affirmation Only assumptions strictly and apply suicide rates that an otherwise uninformed person might assume from the widespread narrative, the suicide myth flunks this rationality test quite badly.
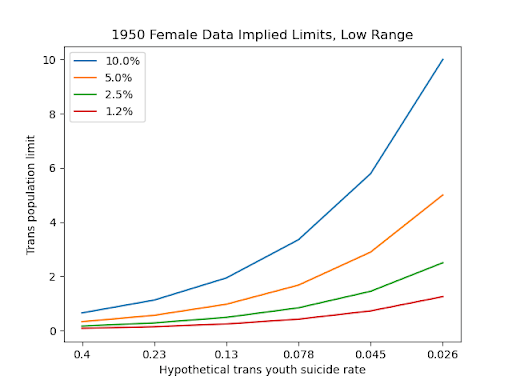
It’s possible to object to particular selections of parameter values in the above computation, but not without making compensating changes elsewhere. To better characterize the feasible space let’s plot the maximum T and S that may be consistent with observed data. The following charts plot values of T along the y-axis against S (over full age 15-24 period) on the x-axis exactly where I=1 for several hypothesized Pt. All values are expressed as percentages. The first chart is based on the observed 1950 female annual youth suicide rate of 2.6 per 100k (0.026% when summed over a 10 year youth period). It plots 4 separate curves corresponding to differing assumptions about the proportion of total youth suicides that could be due primarily to transgender distress. If we assume this is the cause of no more than 10% of all female youth suicides, then the transgender population can be no larger than 0.6% of the whole female population, unless its youth suicide rate is also less than 0.4% which is at least 100 times lower than the widely cited “suicidality” claim.

The next chart extends these curves to the right showing bounds on feasible values if the innately transgender part of the female population is 1% or above. The overall female youth suicide rate is 0.026% when summed over the age 15-24 decade, and each curve shows a trans population limit equal to the total trans suicides limit when the trans youth suicide rate exactly matches the overall youth suicide rate. Observe that for plausible (i.e. < 10%) estimates of the proportion of all youth suicides that are primarily due to transgender distress, if the total trans population is anywhere near 1% its true suicide rate can be no more than a modest multiple of the full poplation rate.
The third chart uses the much larger observed overall suicide rate of 17.1 per 100k for males in year 2000, in case one objects that the 1950 female rate is inapplicable. Using this value and assuming that 5% of all male youth suicides are by trans youth allows that 1% of the male population could be transgender if their 10-year youth suicide rate is about 0.76% or below.
Keep in mind that this is only 4.5 times the overall male rate.
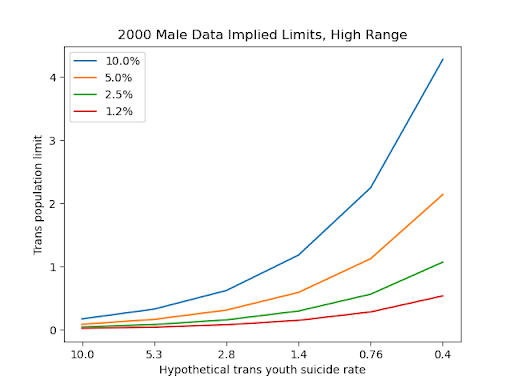
The prior chart was generous to the trans suicide myth by entertaining speculation that a substantial portion of one of the higher documented suicide rates (US males) might be primarily motivated by transgender distress, despite there being no more than a comparatively tiny number of documented suicides of known transgender people. If one fails to make the effort to investigate more deeply, it’s easy to assume that large numbers of a generic phenomenon could be hiding a substantial fraction of a specific phenomenon that one intuitively believes should exist. However, a strong interpretation of the AO hypothesis requires that its tenets also hold across time, geography and culture, in circumstances where the documented suicide rates are much lower. Reported suicide rates vary dramatically across nations, suggesting that predominant causes are in part cultural. Among the EU nations Greece has consistently had among the lowest rates. In 2019 their national rate was 2.4 (3.7 male, 1.0 female), even lower than the 1950 US rates. Intriguingly, some tropical and island nations consistently record even lower rates. The Philippines reports an overall rate around 2.2, while a number of Caribbean nations collectively report a rate around 1.0.23 Could it be that warm, sunny weather and strong family and community bonds are more effective in relieving transgender distress than hormones and surgery? Calculating with R=1.0, T=5%, S=4%, Pt = 5% yields an extreme infeasibility factor of 400.
In summary, it is not plausible that 1% or more of the population is innately transgender and always has been, and that this population exhibits an extremely high completed suicide rate (i.e. 10 times or more the US general rate) unless granted social affirmation and medical transition. That conjecture is grossly inconsistent with historical and cross-national data. The only parameter values consistent with the data assume either that transgender people are vanishingly rare (as was believed prior to roughly year 2000), or their true youth propensity to suicide is not much greater than that of other youth with recognized psychological problems.
Suicide, Suicidality and Performative Exhibitions of Despair
Suicide is a serious topic, so it should be discussed seriously, which is to say with complete honesty and with greatest respect for unambiguous and replicable empirical evidence. In particular we should acknowledge that the factors that lead someone to take their own life are probably as complex, poorly understood, and unique to the individual as any topic in human psychology. Simple and sweeping hypotheses about the cause of unhappiness or self-harm in a group of superficially similar people should be subject to strong skepticism.
We should also acknowledge that actual suicide and the range of behaviors that are sometimes described as “suicidality” are not expressions of a single, simple phenomenon, distinguished only by intensity. The factors that lead to a completed suicide can be substantially different from those that lead to outspoken suicidal ideation or performative “attempts” like shallow cutting. There has been much study of suicide for decades, and still little insight into how to reliably predict an individual suicide. There seems to be an impulsive, opportunistic element to many suicides. A simple self-report of past suicidality gives very little predictivity of eventual completed suicide.24 It’s been shown that people self-report suicide attempts inconsistently.25 Although some believe that self-report of a suicide attempt is a robust predictor of (more likely than average) future suicide, one study has shown that measures of suicidality in adolescents may not only not be predictive of actual suicide, but not even predictive of later suicidality either.26 It is very difficult to know how to interpret self-reports of having attempted suicide. Studies vary in the degree to which they attempt to distinguish between serious and more casual or loosely interpreted attempts. It’s known that the ratio of reported attempts to completions differs dramatically between demographic groups. For example, in the US females are thought to attempt suicide at roughly twice the rate of males, but males actually die by suicide at a three to four times higher rate.27 It seems plausible that even more extreme differences may exist among more finely differentiated subgroups. It is also known that both suicides and Non-Suicidal Self Injury (NSSI; performative suicidality) are subject to considerable social and peer influence. For example, adolescent suicides often occur in clusters28 and NSSI clusters in friend groups.29
In recent years there were two highly influential research reports published that are purported to show outsized suicide risk in trans identified youth. The first was the 2011 National Transgender Discrimination Survey report, which headlined a claim that “a staggering 41%” of transgender people attempt suicide. This survey and report were the product of a trans-advocacy group, the National Center for Transgender Equality. That group was founded in 2003, around the time of the transactivist shakeup in which the HBIGDA transformed into WPATH. The report’s claims were widely trumpeted by various aligned activist groups whose representations were then repeated by the popular media. Google scholar shows over 3000 citations for the report, indicating its success in influencing subsequent discussion. The NTDS was the origin of the now widely cited 41% statistic. The second was a 2018 paper published in Pediatrics titled Transgender Adolescent Suicide Behavior (Toomey et al.) that reported suicide attempt rates from 30% to 50% for subcategories of transgender identified youth. Although it appeared in a publication of the American Academy of Pediatrics, the authors were not medical researchers but rather unaffiliated minor academics from newly invented social science disciplines with strong social justice orientations. Coincidentally, it appeared in the same issue of Pediatrics as the Rafferty authored AAP position paper expressing support for Affirmation Only. The Toomey paper too was uncritically embraced and echoed by much of the media, which treated its appearance in a medical journal as scientific confirmation of the earlier NTDS report, and justification for Affirmation Only policies. For example, the Human Rights Campaign reported, “Harrowing statistics from a study recently published by the American Academy of Pediatrics revealed alarming levels of attempted suicide among transgender youth.”
Studies based on surveys are subject to a variety of biases and weaknesses that call for caution in accepting their conclusions, and these two are not exceptions. However, it’s not necessary to criticize them at that level of detail in order to understand their essential lack of support for the suicide myth. Their major shortcomings are right on the surface: the difference between self-reported suicidality and real likelihood of completed suicide, and attribution of causality.
The Toomey paper found that survey respondents reported having attempted suicide at the following rates, according to reported gender identity.
| gender id: | male | female | not-sure | MtF | non-binary | FtM |
| count: | 57871 | 60973 | 1052 | 202 | 344 | 175 |
| rate: | 9.8% | 17.6% | 27.9% | 29% | 41.8% | 50.8% |
The rates for male and female are not more than a factor of 2 different from those reported by the CDC Youth Risk Behavior Survey Data Summary & Trends Report: 2011-2021 which had a different methodology and questions, so they seem roughly plausible. How do these reported attempts compare to known completions? The surveyed students’ age averages perhaps 16 at oldest, so 4x the youth range average risk is probably an okay estimate for actual cumulative suicides of their age-matched cohort. The 2014 recorded rates were 4.8/100k for female youth and 18.2 for males. That yields a ratio of 17.6%/(4 * 4.8/100000) = 917 to 1 for females, and 9.8%/(4 * 18.2/100000) = 135 to 1 for males. In other words, for every 900 females reporting a suicide attempt, perhaps one in that cohort had actually died by suicide. Among males the rate of completions per reported attempt was nearly 7 times higher.
It’s tempting to assume that greater rates of reported suicide attempts correspond to greater unhappiness and greater likelihood of dying by suicide. Yet the striking inversion of report rates versus completion rates for males and females begs questions of the following kind: Are females really unhappier than males, or just more inclined to demonstrate unhappiness in this way? Is there more than one kind of unhappiness that might prompt a reported attempt, but only some of those kinds that are likely to result in a completion? How can we guess the completion predictability of the various transgender categories; are they more like male ratios or female ratios? Given the small size of the subpopulations reporting transgender identities, is it plausible that their reported-to-completion ratios are higher or lower than either males or females? Neither of the two papers mentioned above address these questions.
The other question begged but not addressed by these two reports has to do with causality: Do transgender identified people report suicidality primarily due to lack of social and medical accommodation, or is it the case that people prone to suicidality for independent reasons also tend to identify as transgender? This question is partially addressed by a more recent multi-clinic study Suicidality in clinic-referred transgender adolescents (de Graaf, et al.), published in 2022. It covered 2771 adolescents seen at gender clinics in the UK, Canada and the Netherlands, between 1978 and 2017. It retrospectively examined patient records for degree of expressed suicidality and correlation with other recorded data. It did not cover all applicants to those clinics, just (some of?) those who clinicians felt met the diagnosis criteria for one of several related DSM definitions for Gender Dysphoria. It also compared their scores with those of otherwise similar youth referred for mental health issues other than GD, and those not referred at all. A brief summary of the results is that the GD adolescents expressed suicidality at substantially higher rates than for youth not referred for mental health, but only slightly higher than those referred for other reasons. It also found that the single highest correlate of suicidality among the GD adolescents was general behavior and emotional problems. Their findings were “consistent with various studies which show that adolescents diagnosed with GD have, on average, a greater number of behavioral and emotional problems in general when compared to non-referred adolescents, but relatively similar to adolescents seen clinically for other types of mental health issues.”
Before and After Transition
Social science is hampered to a large degree by the difficulty of obtaining high-quality data that clearly discriminates between competing hypotheses. For ethical as well as practical reasons it is impossible to conduct controlled experiments that directly address many interesting questions. Often researchers need to wait for observational data to accumulate slowly in consequence of whatever societal trends happen to play out, then painstakingly attempt to identify causal relations out of a myriad of potentially confounding factors. This is something to keep in mind whenever it is claimed that some social or medical theory is “settled science.”
Practitioners of gender medicine have boldly acted on novel theories in advance of strong empirical support. Back when transsexuals were considered a 1 in 40,000 anomaly, the phenomenon was difficult to study and of little general interest or ethical concern. Now, following explosive growth in the number of clinics and patients, data is starting to accumulate. So far there have been few studies reporting on actual suicides among transgender people, mostly on an anecdotal basis. I know of only three where the numbers are large enough to begin to be statistically meaningful, though still only weakly so. One examines suicides among adolescent gender clinic patients in the UK. The other two look at long term outcomes of mostly adult patients in the Netherlands and Sweden.
Suicide by Clinic-Referred Transgender Adolescents in the United Kingdom (Michael Biggs, 2022) analyzed suicides among adolescent patients of the Tavistock Gender Identity Service (GIDS) between 2010 and 2020. Since the number of patients applying to GIDS grew dramatically30 during that period, the median patient was effectively tracked for only about 2 years. During the years covered 4 suicides were reported, all between 2017 and 2020. Two of the patients were on the waiting list and had not yet been seen, two had already been seen and begun treatment. Meanwhile around 15,000 patients applied to the service. In aggregate about 30,000 patient years were tracked, so scaling up yields an annual rate of 13 suicides per 100k. Weighting for the predominantly female population of GIDS patients, this is 5.5 times the rate for UK adolescents in general. However, given the tiny number of suicides the exact multiple is a low confidence number, approximating the suicide risk of adolescents with other mental health issues. Biggs writes, “The proportion of individual patients who died by suicide was 0.03%, which is orders of magnitude smaller than the proportion of transgender adolescents who report attempting suicide when surveyed. …It is irresponsible to exaggerate the prevalence of suicide. Aside from anything else, this trope might exacerbate the vulnerability of transgender adolescents.”
The Netherlands was one of the first countries to provide transsexual services within its national healthcare system. An advantage of a national system is that it can make tracking long term outcomes across the population much easier. In 2017 Wiepjes et al.31 surveyed the charts of all referrals to their Amsterdam clinic between 1972 and 2017, including children and adults. Out of 8263 patients identified there had been 49 deaths (0.6%) by suicide. By their measure the suicide rate was about 3 to 4 times that of the general Dutch population, matching for sex but no other demographic factors. (The authors did not attempt to correct for duration skew due to the exponential increase in the number of new patients in recent years.) Notably, the suicides occurred at every stage of transition but mostly well after the fact. The median time between starting cross-sex hormones and suicide was over 6 years. The authors point out that the Netherlands is among the most socially supportive societies with respect to transgenderism. This study suggests that whatever other benefits it may have, medical transition may not significantly reduce suicide risk in this population. Similar results were found in 2011 by an earlier Dutch study32 covering many of the same patients.
Another European country with a national healthcare system and early support for transsexual medicine was Sweden. In 2011 Dhejne et al.33 performed a similar chart study of all 324 patients who had received sex reassignment between 1972 and 2003 in Sweden (which required surgery for reassignment during that period). For each transsexual identified, the authors selected 10 random other Swedish medical records of each sex matched for age against which to compare health outcomes. Their comparison found that overall mortality was significantly worse for transsexuals. The largest cause of death was suicide, followed closely by cardiovascular disease. The measured suicide rate was 19 times greater than the control group. Psychiatric hospitalization was also 3 times greater than in the control group, even after excluding hospitalizations for Gender Dysphoria. Interestingly, the Kaplan-Meyer curve shows that the mortality curves for the transsexuals are close to those of the controls for the first 10 years, after which the transsexuals fared much worse.
Together, the Dutch and Swedish studies just described suggest both that medical transition does not reduce suicide risk and that very long term follow up (20 years or longer) is necessary to understand the true health outcomes of gender medicine interventions.
Concluding Thoughts
Exaggerating the risk of suicide in transgender identified youth is a deliberately manipulative tactic that persists because it too often works. It works as emotional blackmail against parents who are frightened by the thought of losing a loved one. It works to intimidate legitimate criticism via inciting opprobrium from the well meaning but uninformed. And it works like a conjuror’s misdirection to distract attention away from the poor science underlying Affirmation Only policies. Propagation of the trans suicide myth should not be engaged in nor tolerated by responsible people who are serious about evidence-driven health care. Medical professionals should have the skills and motivation to read the relevant literature and understand its implications.
- The risk of completed suicide in transgender identified youth may be higher than average for all youth, but not by a large factor and probably not greater than that of youth with other psychological disorders that are common co-morbidities among the trans identified.
- There is no evidence that long-term real suicide rates are lowered in this population by medical transition.
- The likely real risk of youth suicide in this population is less than the likelihood of permanent health damage and regret later in life.
Notes
- The rise and fall of gender identity clinics in the 1960s and 1970s | The Bulletin
- Both the Placebo Effect and the Hawthorne Effect can confound experiments on humans. In the first case a subject’s belief in the efficacy of treatment can lead to a positive outcome even where the treatment is otherwise ineffective. In the second case a subject’s awareness that they are being observed can encourage greater self awareness and self reflection, leading to altered behavior and a better outcome. Consultative interaction with medical professionals not involving surgery may have had direct or indirect therapeutic effects of this kind. These are among the reasons why studies showing improvement correlated with administration of a treatment that don’t also compare a similarly handled but untreated control group should be regarded skeptically.
- The first major medical society to publish a guideline in support of medical transition was the Endocrine Society in 2009 with Endocrine Treatment of Transsexual Persons:An Endocrine Society Clinical Practice Guideline. That paper credited 8 authors of whom 3 had previously served as officers of WPATH (Cohen-Kettenis, Gooren, Meyer), 2 others have served on WPATH committees (Hembree, Tangpricha) and 2 others were founders of early gender clinics treating minors (Delemarre-van de Waal, Spack). That paper set in motion subsequent endorsements by other societies who assumed good faith and competence on the part of the Endocrine Society. The next highly influential society endorsement was the 2018 AAP position paper Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and Adolescents that promoted the Affirmation Only approach for youth. It was authored almost entirely by a single young doctor just out of residency and it cited WPATH publications in many places. This paper’s systematic misinterpretation of other cited papers was documented in Transgender and Gender Diverse Children and Adolescents: Fact-Checking of AAP Policy
- There are many personal accounts on the internet by parents attesting to the use of this tactic by AO advocates, including licensed therapists and doctors. Also see Jamie Reed’s Affidavit to the State of Missouri testifying that doctors at a St. Louis gender clinic often used this tactic on skeptical parents.
- Suicidality is known to be socially contagious. Promoting the idea that a self-diagnosed condition is associated with elevated suicidality is grossly irresponsible. The infamous doctor Wallace Wong of Vancouver who has ‘treated’ an extraordinary number of supposedly transgender foster care youth was recorded describing how he coaches youth to claim suicidality. Wallace Wong: Exposed
- The power of 41%: A glimpse into the life of a statistic
- Impacts of Strong Parental Support for Trans Youth
- NIMH » Mental Health Research—Diversity Matters
- Risky Behavior Among Youths: An Economic Analysis
- https://www.statista.com/statistics/1114191/male-suicide-rate-in-the-us-by-age-group/
- https://www.statista.com/statistics/1114127/female-suicide-rate-in-the-us-by-age-group/
- https://www.ncbi.nlm.nih.gov/books/NBK569311/table/ch3.tab9/
- An analysis of all applications for sex reassignment surgery in Sweden, 1960-2010: prevalence, incidence, and regrets
- An analysis of all applications for sex reassignment surgery in Sweden, 1960-2010: prevalence, incidence, and regrets
- How many people are lesbian, gay, bisexual and transgender?
- Race and Ethnicity of Adults Who Identify as Transgender in the United States
- https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/
- About 5% of young adults in U.S. are transgender or nonbinary | Pew Research Center
- The Emergence of Youth Suicide: An Epidemiologic Analysis and Public Health Perspective
- Explaining the Rise in Youth Suicide
- Risk Factors, Assessment, and Treatment of Adolescent and Young Adult Suicidal Patients – ScienceDirect
- Full article: Suicide and Suicide Risk in Lesbian, Gay, Bisexual, and Transgender Populations: Review and Recommendations
- WHO: World Suicide Rates
- Self-reported life-weariness, death-wishes, suicidal ideation, suicidal plans and suicide attempts in general population surveys in the north of Sweden 1986 and 1996
- Demographic and Clinical Characteristics of Consistent and Inconsistent Longitudinal Reporters of Lifetime Suicide Attempts
- Diagnostic outcome of adolescent self-reported suicidal ideation at 8-year follow-up
- https://www.nimh.nih.gov/health/statistics/suicide
- Suicide Clusters: A Review of Risk Factors and Mechanisms
- Peer Socialization of Non-Suicidal Self-Injury in Adolescents’ Close Friendships – PMC
- https://segm.org/images/280.UK_full.svg
- Trends in suicide death risk in transgender people: results from the Amsterdam Cohort of Gender Dysphoria study (1972–2017) – Wiepjes – 2020 – Acta Psychiatrica Scandinavica
- A long-term follow-up study of mortality in transsexuals receiving treatment with cross-sex hormones
- Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden
{kind=link}