Three Strategies to Respond to an Ideological Crisis
By Stella O'Malley and Levi Pay
In the field of so-called “gender medicine”, we have seen a shameful abdication of responsibility that has left the public confused and misled. This is a continuing scandal that is at once medical, cultural, and institutional.
In the vacuum left by failed institutions, others have stepped in to understand, expose, and address the scandal. Three primary strategies have emerged, each with its own strengths and its own limitations or flaws.
Unapologetic honesty about the harms of medical transition and trans ideology is at the heart of all three approaches, but how that honesty manifests is quite different in each case.
What are the three approaches and how do they fit together? Do they support or contradict one another? What might all this mean for where we go next?
Most people – the unengaged public, as well as your average lawmaker or policy-maker – presume there are elements to “being trans” that are difficult to understand. They assume that experts have studied the field and that the lack of evidence reflects science not yet catching up, rather than the consequence of elaborate efforts to promote shoddy research that encourages heavy-handed interventions.
Yet anyone who has studied the literature knows there is no quality evidence to justify medicalising the identities of minors whose identities are still in mid-formation. That part is not really in dispute.
What differs is how people respond to this reality and how we address the central dilemma: that most people mindlessly follow the herd. It turns out that the majority of people concede authority to others on any given issue, even against their better judgement. Most of us seek an easy life and trans feels just too difficult an issue for most people.
A startling lack of integrity and courage has run through medicine, psychiatry, counselling, law, academia, and journalism. Mental health professionals did not set firm boundaries decades ago when they had the opportunity and, since then, field after field followed suit.
Ideology displaced judgement. Medicine and academia gave the ideology false authority, law and policy enshrined it, journalism became a cheerleader instead of a watchdog, mainstream feminism traded hard-won insights for identity politics, and the mainstream gay rights movement shifted from defending same-sex attraction to embracing trans ideology.
Amid a moral crisis in society, every profession faces a choice. Journalists must decide whether to be watchdogs or bystanders. Doctors must choose between protecting patients or protecting their careers. Academics must either challenge bad science or hide behind a false – and often enforced – consensus. The list goes on, but essentially, for responsible professionals, the question is stark. Stay silent and let lies take root, or speak out and say, “No, this reckless medical practice must end.”
As institutions faltered and left a void, some determined individuals and groups rose to the challenge – taking on the vital work that had been neglected. In striving to understand, reveal, and confront the scandal, three distinct and dynamic strategies came to the fore.
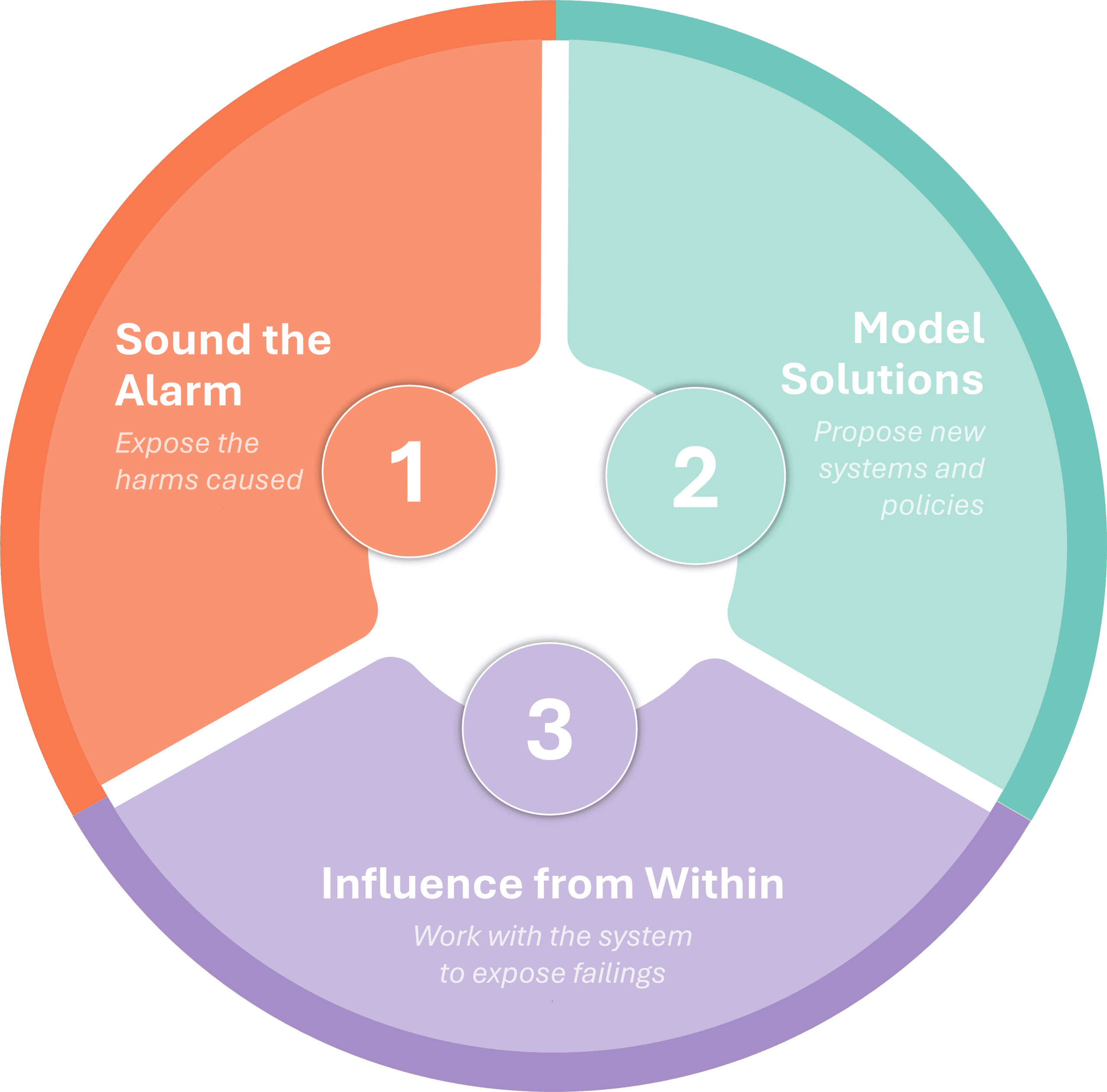
Sound the alarm
Sound the alarm is an approach which centres on raising public awareness of the harms caused by trans activists and their allies as loudly and as publicly as possible. These harms relate to the serious and often lifelong harms that come with medical transition, as well as the harms inflicted on women’s rights, children’s rights, freedom of speech, and academic freedom more broadly.
This is a vital strategy when our institutions do not know, or pretend not to notice, what is playing out right in front of them. Although these campaigners are often worlds apart politically – and, on occasion, even bitterly opposed to one another, they share a strikingly similar approach.
With tactical similarities, they might be seen by some – particularly by casual observers and newcomers – as a single, unified front, marching in the same direction and successfully forcing a set of issues into the public eye. Their different, or even contradictory, motivations will often be better understood by those more familiar with the issues.
What are the risks of the sound the alarm approach? One potential risk is that the disengaged majority may dismiss it as little more than online hostility. Even when the strategy succeeds in raising the public profile of these issues, some observers who see themselves as centrist or mainstream may feel turned off by the intensity and the heightened emotion being expressed.
The directness of this approach might also attract support from trolls or thugs – people who are more interested in a fight – any fight – than they are in this particular fight for the rights of children, women, medical ethics or free speech. Their support, often lent from behind anonymous social media accounts, can further confirm some of the unhelpful suspicions held by bystanders.
Model solutions
The second strategy to model solutions is adopted by organisations and commentators who are united by a commitment to refocus laws, redirect regulations and policymaking, and reform institutional and professional practice. The group is no less diverse than those who sound the alarm; the individuals and organisations seeking to model solutions also have very different motivations, priorities, and perspectives, resulting in a rich array of approaches to address the issues at hand.
The bread and butter of those modelling new approaches is hard policy graft. Whether proposing amendments to statute law, giving oral testimony in our legislatures, writing and publishing new frameworks for medical practice, arranging conferences, submitting consultation responses, or writing books, this approach is about analysis – presenting evidence, without equivocation, and promoting a vision for how we can move forward.
By proposing reforms and modelling constructive alternatives, the people in this group can be tricky for institutions and politicians to dismiss or ignore – especially once it becomes clear they are in this for the long haul and not going anywhere.
While this all sounds very positive, this approach, like all strategic approaches, has its downsides.
While the proponents of this approach like to model what is happening, we also need to accept that, in many ways, it was analysing and modelling these issues that helped get us into this quagmire in the first place. Academics, including academic clinicians, can find themselves analysing or feeding a crisis, even as it grows more every year. The flowery or technical language of academia can cushion academics and clinicians from the harsh reality of what is happening, or give harmful practices an unearned air of respectability and academic endorsement. Those seeking to model new solutions need to be careful not to fall into similar traps – for example, by engaging in endless analysis without presenting clear solutions or by putting forward solutions which are insufficiently analysed or evidenced but which, nevertheless, become entrenched.
Those demonstrating this second approach can also find themselves in an awkward middle – criticised as insufficiently radical by the sound the alarm crowd and, simultaneously, seen as too blunt and dismissive by those who favour a more consensus-building approach (about whom more later).
Solution-focused policy work is easily dismissed as dull (just typing the words “solution-focused policy work” in this article feels like it should be accompanied by an eyeroll) or, worse, as appeasement. Someone willing to attend a government roundtable discussion or speak at a conference on a panel, alongside people and organisations who fundamentally disagree with their position might come across as being too open to compromise, even when their policy lines are straightforward.
At the same time, their clarity means their position can still be dismissed as too extreme by those new to the issues, including many who hold power within our institutions. The mud slung several years ago of “hate group” might not stick today in quite the same way as it did, but it can still make the job of influencing policy feel Sisyphean at times.
Influence from within
The third strategy to influence people and institutions on these issues treats engagement with gender-affirmative clinicians and pro-trans advocates as a key aspect of moving forward – a premise that ignores overwhelming evidence to the contrary.
On the upside, this approach can reach audiences who might otherwise dismiss more challenging voices. Those taking this approach may gather certain types of evidence – interviews, case studies, and whistleblower testimony – that require building trust with insiders. The BBC’s Newsnight investigations into GIDS at the Tavistock and Portman NHS Foundation Trust (in 2019 and 2020), or the US television show 60 Minutes piece on detransitioners (in 2021), likely benefited from individuals willing to work within institutional constraints. But these minor victories come at a cost.
A possible weakness of this approach is that it might reinforce some aspects of the frameworks it is challenging. This strategy might treat, for example, certain types of language and ideological concessions as a necessary price of entry; inconvenient truths could be avoided.
The Cass Review should have been the turning point; a comprehensive, damning analysis of paediatric “gender-affirming care.” The UK’s Gender Identity Development Service (GIDS) at the Tavistock and Portman NHS Foundation Trust was closed. The scandal was laid bare. From this point on, clarity was required. Yet leadership faltered. Clinicians remained equivocal, few willing to state clearly that this was a harmful intervention that should never have been described as healthcare. Children should not be subjected to needless experimental medication yet the Cass Review recommended the £10m publicly funded puberty blocker trial that subjects further children to unnecessary and harmful medical interventions – despite the commissioned systematic reviews finding no evidence of benefit and documenting significant harms.
The reformist stance can assume that the institutions they work with share their commitment to evidence and ethics – an assumption the facts have long since demolished. The WPATH Files, leaked internal communications from the World Professional Association for Transgender Health whose standards guide gender clinics globally, revealed members admitting children are “nowhere in any kind of brain space” to understand fertility risks, yet continuing to promote treatments. Court documents from Alabama’s legal challenge showed WPATH suppressing unfavourable evidence reviews and working with legal advisors to shape guidelines for court victories rather than patient care. Despite these revelations, WPATH faces no meaningful institutional consequences – medical associations still cite their guidelines, universities still host their conferences. We need to be wary of the risks, as well as any potential benefits, of working with organisations that have caused such harm.
How do the three approaches fit together?
Broadly, these are three different ways to understand, expose, and address the harms that arise from “gender-affirming” approaches to medicine and from the broader belief that people’s subjective gender identities should take priority over their sex. We say ‘broadly’ because, of course, many dip in and out of the three approaches at different times, depending on the context, the audience, or the specific point being made.
This overlap matters. Each of these strategies has real merit, and each comes with genuine limitations. What’s important is that we recognise and appreciate this – that we resist the temptation to elevate one approach as the only legitimate path while dismissing the contributions of others.
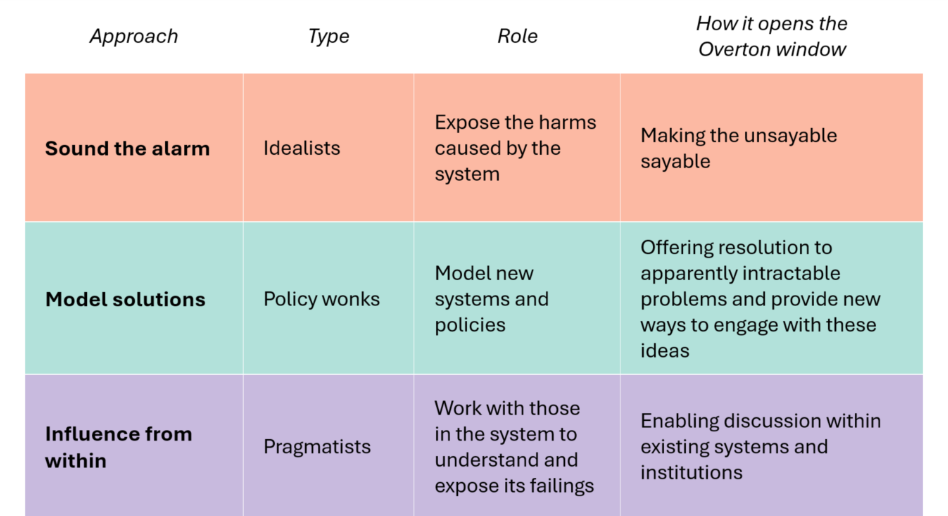
Yet it is easy, particularly in polarised and volatile times, to dismiss those who take a different approach to our own. If we consider how the Overton window has been opened, with space created for open discussion and debate on these issues in a way that seemed impossible just a few years ago, we must acknowledge that contributions have been unequal, both in effect and in cost.
Sound the alarm helped to make the unsayable sayable, often through people bravely setting their own examples.
The people and organisations seeking to model solutions gave those whose role it is to shape laws, policy and professional practice new frameworks for engaging with these ideas.
Those preferring to influence from within secured wins within existing systems and institutions.
These divergent approaches inevitably generate friction, yet such internal disagreement has proven valuable. It hones our arguments, challenges our thinking, forces us to refine our positions. Particularly when your opponents have suffered from a distinct lack of this sort of internal challenge – trapped in enforced consensus – the intellectual rigour that comes from genuine debate becomes a significant advantage.
The arguments are far from over. A year and a half after the Cass Report was published, NHS clinicians remain uncertain about how to understand, treat, or even speak about gender dysphoria, private clinics are cashing in, and legislation on conversion practices, which will carry potentially harmful unintended consequences, is still being pushed through in some of our legislatures. Those arguing for “gender-affirming care” increasingly resort to emotional manipulation and legal threats, having abandoned any pretence of scientific credibility. The evidence vacuum at the heart of their movement becomes more glaring with each passing month.
What of the future?
We find ourselves at an interesting inflexion point. One side of this issue is in the process of being exposed, at the level of the US Supreme Court no less, as having no compelling evidence in support of its arguments. The other side – our side – is finding that the stacking evidence in our favour only gets us so far when institutions refuse to acknowledge it.
The most effective strategy has been for trans activists to present gender distress as a human rights issue. If being trans is framed as akin to being gay, evidence becomes secondary and the assumption of being born this way pushes data to the margins.
But the science in this field is not simply weak. It was never there, and you cannot prove a negative. Those who know the field recognise that high-quality evidence will never emerge because the entire premise rests on unfalsifiable claims about inner identity. We already have our answer, stated repeatedly, that the evidence ranges “from low to very low certainty.” No amount of research can validate a category error.
Rigorous research must continue because it generates the solid knowledge base that this field has always lacked, but alone it will not shift the culture. As Cori Cohn stated at the recent Genspect conference, “In the debate over trans medicine, evidence is no longer relevant…narratives have always dominated the facts”.
It is tempting to think that we may not always have the same need for all three approaches if we continue to turn things around in the way we are doing – and yet it is premature to think we can dispense with any of the approaches anytime soon.
All three approaches are key to generating and promoting the powerful narratives we need in so many ways. It is precisely the synergy of sounding the alarm, modelling solutions, and influencing from within that has prised open the Overton window and driven change. As we continue the slow, stubborn task of restoring faith in evidence and in our institutions, we must hold our nerve and keep every tool at hand.
This improved version was written in collaboration by Stella O’Malley and Levi Pay and reflects a clearer and more balanced understanding than the earlier article. We apologize for any unintended impact.